
MCC eCare Plan Implementation Guide
1.0.0-ballot2 - ballot
![]()
MCC eCare Plan Implementation Guide
1.0.0-ballot2 - ballot
![]()
This page is part of the MCC eCare Plan Implementation Guide (v1.0.0-ballot2: STU 1 Ballot 2) based on FHIR (HL7® FHIR® Standard) R4. The current version which supersedes this version is 1.0.0. For a full list of available versions, see the Directory of published versions
| Official URL: http://hl7.org/fhir/us/mcc/StructureDefinition/mccCarePlan | Version: 1.0.0-ballot2 | |||
| Active as of 2022-04-13 | Computable Name: MCCCarePlan | |||
This profile constrains the FHIR Care Plan Resource to represent the requirements of a care plan for patients with multiple chronic conditions.
A Care Plan is a consensus-driven dynamic plan that represents a patient’s and Care Team Members’ prioritized concerns, goals, and planned interventions. It serves as a blueprint shared by all Care Team Members (including the patient, their caregivers, and providers), to guide the patient’s care. A Care Plan integrates multiple interventions proposed by multiple providers and disciplines for multiple conditions. A Care Plan may represent one or more Care Plans and serves to reconcile and resolve conflicts between the various plans developed for a specific patient by different providers. It supports the following use cases:
The vision of this implementation guide (IG), with the FHIR Care Plan profile as its framework, is to define a profile on the FHIR Care Plan resource that describes how it can be implemented and leveraged to support machine assisted care coordination between systems. It is assumed that clinician and patient facing SMART on FHIR Apps can be designed off of this guide to achieve that goal. The IG will also inform EHR systems on how to implement a structured encoded Care Plan.
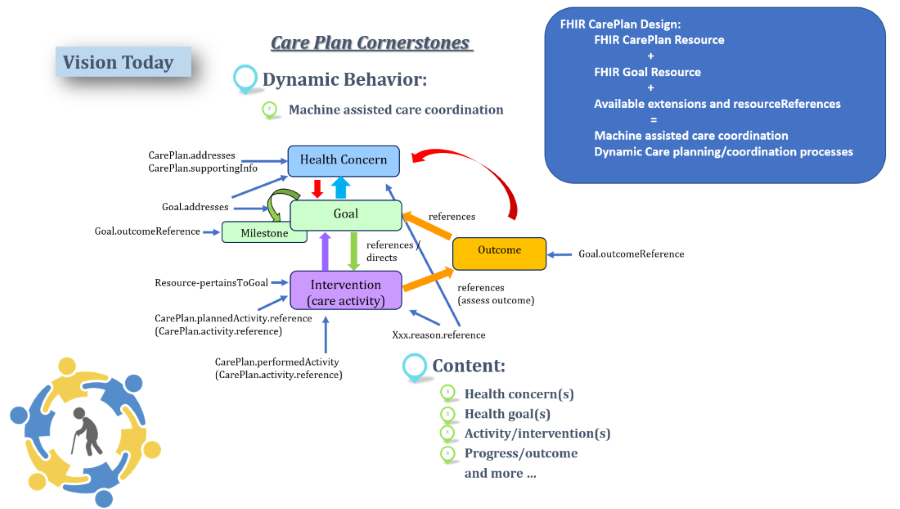
The dynamic care plan process diagram shows Care Plan Cornerstones as they exist within the clinical world and elements and attributes from the FHIR Care Plan resource structure that support the process. In order to encourage reuse and dynamic, machine assisted care coordination, the Care Plan profile design leverages referrencing profiles wherever possible, especially within CarePlan.Activity.
 |
This profile on the FHIR Care Plan Resource describes rules and contraints to record, search, and fetch care plan data associated with a patient with multiple chronic conditions. It identifies which profiles, core elements, extensions, vocabularies and value sets SHALL be present in the resource when using this profile. Care plan data may or may not be tagged in an EHR as part of a care plan, but is also useful to retrieve data such as goals, problems, medications etc. and their time stamps from EHRs and other health system records to bring into an aggegated plan. This includes care plans that may be authored by a patient.
 |
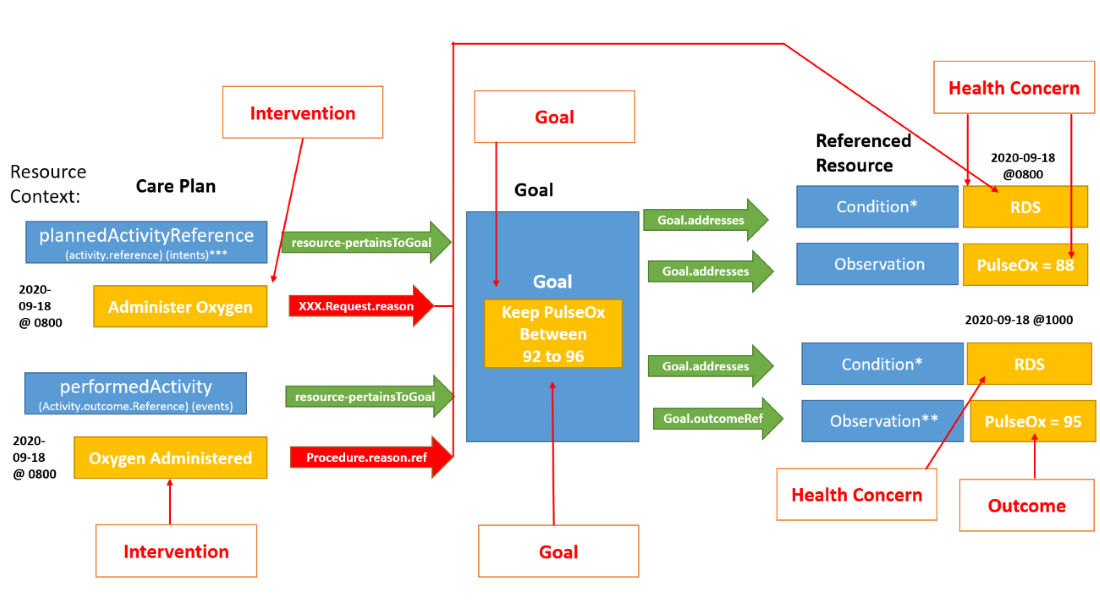
The machine assisted dynamic care planning/coordination is supported in FHIR by leveraging together the Care Plan resource, the Goal resource, resource referencing and available extensions within those resources to “link together the health concern or problem, and it’s associated goals, interventions and outcomes. The intention is to re-use data entered in the EHR, whether it is in a Care Plan Application, or elsewhere in the EHR or other information system, rather than having a care plan be a double documentation burden. For example, if a procedure is ordered and performed and the health concern or problem reason for that procedure is asserted in the ordering workflow or documentation workflow - this information can be pulled into the Care Plan. If a goal is asserted for a patient outside of a care plan, along with the reason for that goal, this also can be pulled into a care plan. The Care Plan profile relies on referencing of profiles rather than “in-line” representation or documentation to enable a dynamic workflow and to be able to pull in and aggregate care coordination activities from disparate systems to provide a comprehensive care coordination view for patients
CarePlan.activity is a Backbone element. It identifies an action that has occurred or is a planned action to occur as part of the plan. For example, a medication to be used, lab tests to perform, self-monitoring that has occurred, education etc., within which in R4 can be activity.reference, activity.outcomeCodeableConcept, activity.outcomeReference or activity.progress (annotated note).
OUTCOME REFERENCE - activity.outcomeReference (aka PERFORMED ACTIVITY reference): has been renamed in R5 to “CarePlan.performedActivity”. To be in line with R5 do not use activity.detail. Also, outcomeReference is not only an outcome but rather an action such as Procedure or an Encounter that was made or occurred or an Observation. Within the target of the CarePlan.activity.outcomeReference, the extension, “resource-pertainsToGoal” SHALL be used to reference this activity’s related goal. Within the resource referenced within CarePlan.activity.outcomeReference, “xxx.reason” SHALL be used to reference the health concern or problem for which the activity is done. CarePlan.outcomeCodeableConcept can also be used to indicate the outcome of an activity, such as patient understanding or lack thereof. It should not duplicate the activity status (e.g., completed or in progress). Simple free text can be used in the OutcomeCodeableConcept if no specific code is available.
ACTIVITY REFERENCE - activity.reference (aka PLANNED ACTIVITY reference): has been renamed in R5 to “CarePlan.plannedActivityReference”. To be in line with R5 do not use activity.detail. Within the target of the CarePlan.activity.reference, the extension, “resource-pertainsToGoal” SHALL be used to reference this activity’s request’s related goal. “xxx.reason” SHALL be used to reference the health concern or problem for which the activity is done. Within the referenced Goal resource, goal.address SHALL be used to reference the goal’s related Condition, Observation, MedicationStatement, NutritionOrder, ServiceRequest or RiskAssessment. Within the referenced Goal resource, Goal.outcomeReference, references the outcome (e.g observations related to the specific goal). Consider using activity.progress, which is an annotation data type, to satisfy the desire in the comment to provide plain free text on progress (in addition to the text, it contains the author and a date-time).
Health Concerns represented with:
Goals represented with:
Interventions represented with:
Outcomes represented with:
 |
Usage:
Description of Profiles, Differentials, Snapshots and how the different presentations work.
This structure is derived from USCoreCarePlanProfile
| Name | Flags | Card. | Type | Description & Constraints |
|---|---|---|---|---|
| 0..* | USCoreCarePlanProfile | Healthcare plan for patient or group | ||
 | ?!Σ | 0..1 | uri | A set of rules under which this content was created |
 | S | 0..1 | Narrative | (USCDI) Text summary of the resource, for human interpretation |
 | S | 1..1 | code | (USCDI) generated | extensions | additional | empty Binding: US Core Narrative Status (required): Constrained value set of narrative statuses. |
 | SC | 1..1 | xhtml | (USCDI) Limited xhtml content |
| 0..1 | Reference(US Core Patient Profile | US Core Practitioner Profile | US Core PractitionerRole Profile | US Core CareTeam Profile | US Core Organization Profile | RelatedPerson | Device | Multiple Chronic Condition Care Plan Care Team) | When populated, the custodian is responsible for the care and maintenance of the care plan. The care plan is attributed to the custodian. The custodian might or might not be a contributor. This CarePlan.custodian extension should be used instead of CarePlan.author which in R4 is currently identified as the designated responsible party and in R5 has been removed. URL: http://hl7.org/fhir/us/mcc/StructureDefinition/custodian | |
| ?! | 0..* | Extension | Extensions that cannot be ignored |
| ?!SΣ | 1..1 | code | (USCDI) draft | active | on-hold | revoked | completed | entered-in-error | unknown Binding: RequestStatus (required): Indicates whether the plan is currently being acted upon, represents future intentions or is now a historical record. |
| ?!SΣ | 1..1 | code | (USCDI) proposal | plan | order | option Binding: CarePlanIntent (required): Codes indicating the degree of authority/intentionality associated with a care plan |
| SΣ | 1..* | CodeableConcept | Care Plan category code describes the type of care plan. Please see CarePlan.category detail for guidance. Slice: Unordered, Open by pattern:$this Binding: CarePlanCategory (example): Identifies what "kind" of plan this is to support differentiation between multiple co-existing plans; e.g. "Home health", "psychiatric", "asthma", "disease management", etc. |
 | SΣ | 1..1 | CodeableConcept | (USCDI) Type of plan Binding: CarePlanCategory (example): Identifies what "kind" of plan this is to support differentiation between multiple co-existing plans; e.g. "Home health", "psychiatric", "asthma", "disease management", etc. Required Pattern: At least the following |
 | 1..* | Coding | Code defined by a terminology system Fixed Value: (complex) | |
| 1..1 | uri | Identity of the terminology system Fixed Value: http://hl7.org/fhir/us/core/CodeSystem/careplan-category | |
| 1..1 | code | Symbol in syntax defined by the system Fixed Value: assess-plan | |
| SΣ | 1..1 | Reference(US Core Patient Profile) | (USCDI) Who the care plan is for |
| Σ | 0..1 | Reference(Patient | Practitioner | PractitionerRole | Device | RelatedPerson | Organization | CareTeam) | Use the CarePlan custodian extension instead. Use of CarePlan.author is discouraged, it is removed in R5. |
| S | 0..* | Reference(US Core Patient Profile | US Core Practitioner Profile | US Core PractitionerRole Profile | US Core CareTeam Profile | US Core Organization Profile | RelatedPerson | Device | Multiple Chronic Condition Care Plan Care Team) | Who provided the content of the care plan |
| S | 0..* | Reference(Multiple Chronic Condition Care Plan Care Team | US Core CareTeam Profile) | Who's involved in plan? |
| S | 0..* | Reference(US Core Blood Pressure Profile | US Core BMI Profile | US Core Body Weight Profile | Multiple Chronic Condition Care Plan Chronic Disease Conditions | Multiple Chronic Condition Care Plan Laboratory Result Observation | Multiple Chronic Condition Care Plan Diagnostic Report and Note | Multiple Chronic Condition Care Plan Procedure | US Core Immunization Profile | Multiple Chronic Condition Care Plan Family History | Document Reference to Patient's Personal Advance Care Plan (Advance Directive) | SDC Questionnaire Response | Multiple Chronic Condition Care Plan Symptom Observation | Multiple Chronic Condition Care Plan Service Request | Multiple Chronic Condition Care Plan Observation SDOH Assessment | Multiple Chronic Condition Care Plan Immunization | Multiple Chronic Condition Care Plan Nutrition Order | Multiple Chronic Condition Care Plan Clinical Impression | Multiple Chronic Condition Care Plan Patient/Caregiver Condition Status Observation | Multiple Chronic Condition Care Plan Questionnaire Response | Multiple Chronic Condition Care Plan Caregiver Considerations Observation | Multiple Chronic Condition Care Plan Clinical Test Observation | US Core RelatedPerson Profile | US Core Observation Occupation Profile) | Please see the libraries of available value sets pertinent for use with the appropriate Multiple Chronic Condition Care Plan Profile for use within the referenced profiles at CarePlan.supportingInfo |
| 0..* | Reference(Multiple Chronic Condition Care Plan Goal) | This Goal represents one or more overarching goal applicable to the entire care plan | |
 | SC | 0..* | BackboneElement | Action to occur as part of plan. This is the backbone element of the care plan that is the root of care coordination activities. While there can be many activities in a care plan, each activity has only one planned.activityRefence |
| ?!Σ | 0..* | Extension | Extensions that cannot be ignored even if unrecognized |
| S | 0..* | Reference(Multiple Chronic Condition Care Plan Procedure | Multiple Chronic Condition Care Plan Laboratory Result Observation | US Core Immunization Profile | Multiple Chronic Condition Care Plan Diagnostic Report and Note | US Core Immunization Profile | Multiple Chronic Condition Care Plan Medication Request | Multiple Chronic Condition Care Plan Chronic Disease Conditions | US Core Body Weight Profile | US Core Blood Pressure Profile | Multiple Chronic Condition Care Plan Goal | US Core BMI Profile | Multiple Chronic Condition Care Plan Symptom Observation) | This CarePlan element represents a PERFORMED ACTIVITY. Please see the libraries of available value sets pertinent for use with the appropriate Multiple Chronic Condition Care Plan Profile for use within the referenced profiles at CarePlan.activity.outcomeReference |
| SC | 0..1 | Reference(NutritionOrder | Multiple Chronic Condition Care Plan Medication Request | CommunicationRequest | DeviceRequest | Task | ServiceRequest | VisionPrescription | RequestGroup | Appointment) | This CarePlan element represents a PLANNED ACTIVITY. Please see the libraries of available value sets pertinent for use with the appropriate Multiple Chronic Condition Care Plan Profile for use within the referenced profiles at CarePlan.activity.reference |
| Documentation for this format | ||||
| Path | Conformance | ValueSet / Code |
| CarePlan.text.status | required | NarrativeStatus |
| CarePlan.status | required | RequestStatus |
| CarePlan.intent | required | CarePlanIntent |
| CarePlan.category | example | CarePlanCategory |
| CarePlan.category:AssessPlan | example | Pattern: assess-plan |
| CarePlan.activity.detail.status | required | CarePlanActivityStatus |
| Id | Grade | Path(s) | Details | Requirements |
| cpl-3 | error | CarePlan.activity | Provide a reference or detail, not both : detail.empty() or reference.empty() | |
| dom-2 | error | CarePlan | If the resource is contained in another resource, it SHALL NOT contain nested Resources : contained.contained.empty() | |
| dom-3 | error | CarePlan | If the resource is contained in another resource, it SHALL be referred to from elsewhere in the resource or SHALL refer to the containing resource : contained.where((('#'+id in (%resource.descendants().reference | %resource.descendants().as(canonical) | %resource.descendants().as(uri) | %resource.descendants().as(url))) or descendants().where(reference = '#').exists() or descendants().where(as(canonical) = '#').exists() or descendants().where(as(canonical) = '#').exists()).not()).trace('unmatched', id).empty() | |
| dom-4 | error | CarePlan | If a resource is contained in another resource, it SHALL NOT have a meta.versionId or a meta.lastUpdated : contained.meta.versionId.empty() and contained.meta.lastUpdated.empty() | |
| dom-5 | error | CarePlan | If a resource is contained in another resource, it SHALL NOT have a security label : contained.meta.security.empty() | |
| dom-6 | best practice | CarePlan | A resource should have narrative for robust management : text.`div`.exists() | |
| ele-1 | error | **ALL** elements | All FHIR elements must have a @value or children : hasValue() or (children().count() > id.count()) | |
| ext-1 | error | **ALL** extensions | Must have either extensions or value[x], not both : extension.exists() != value.exists() | |
| txt-1 | error | CarePlan.text.div | The narrative SHALL contain only the basic html formatting elements and attributes described in chapters 7-11 (except section 4 of chapter 9) and 15 of the HTML 4.0 standard, <a> elements (either name or href), images and internally contained style attributes : htmlChecks() | |
| txt-2 | error | CarePlan.text.div | The narrative SHALL have some non-whitespace content : htmlChecks() |
| Name | Flags | Card. | Type | Description & Constraints | ||||
|---|---|---|---|---|---|---|---|---|
| 0..* | USCoreCarePlanProfile | Healthcare plan for patient or group | ||||||
| Σ | 0..1 | id | Logical id of this artifact | ||||
| Σ | 0..1 | Meta | Metadata about the resource | ||||
| ?!Σ | 0..1 | uri | A set of rules under which this content was created | ||||
| 0..1 | code | Language of the resource content Binding: CommonLanguages (preferred): A human language.
| |||||
| S | 0..1 | Narrative | (USCDI) Text summary of the resource, for human interpretation | ||||
| 0..1 | string | Unique id for inter-element referencing | |||||
| 0..* | Extension | Additional content defined by implementations Slice: Unordered, Open by value:url | |||||
| S | 1..1 | code | (USCDI) generated | extensions | additional | empty Binding: US Core Narrative Status (required): Constrained value set of narrative statuses. | ||||
| SC | 1..1 | xhtml | (USCDI) Limited xhtml content | ||||
| 0..* | Resource | Contained, inline Resources | |||||
| 0..* | Extension | Extension Slice: Unordered, Open by value:url | |||||
| 0..1 | Reference(US Core Patient Profile | US Core Practitioner Profile | US Core PractitionerRole Profile | US Core CareTeam Profile | US Core Organization Profile | RelatedPerson | Device | Multiple Chronic Condition Care Plan Care Team) | When populated, the custodian is responsible for the care and maintenance of the care plan. The care plan is attributed to the custodian. The custodian might or might not be a contributor. This CarePlan.custodian extension should be used instead of CarePlan.author which in R4 is currently identified as the designated responsible party and in R5 has been removed. URL: http://hl7.org/fhir/us/mcc/StructureDefinition/custodian | |||||
| ?! | 0..* | Extension | Extensions that cannot be ignored | ||||
| Σ | 0..* | Identifier | External Ids for this plan | ||||
| Σ | 0..* | canonical(PlanDefinition | Questionnaire | Measure | ActivityDefinition | OperationDefinition) | Instantiates FHIR protocol or definition | ||||
| Σ | 0..* | uri | Instantiates external protocol or definition | ||||
| Σ | 0..* | Reference(CarePlan) | Fulfills CarePlan | ||||
| Σ | 0..* | Reference(CarePlan) | CarePlan replaced by this CarePlan | ||||
| Σ | 0..* | Reference(CarePlan) | Part of referenced CarePlan | ||||
| ?!SΣ | 1..1 | code | (USCDI) draft | active | on-hold | revoked | completed | entered-in-error | unknown Binding: RequestStatus (required): Indicates whether the plan is currently being acted upon, represents future intentions or is now a historical record. | ||||
| ?!SΣ | 1..1 | code | (USCDI) proposal | plan | order | option Binding: CarePlanIntent (required): Codes indicating the degree of authority/intentionality associated with a care plan | ||||
| SΣ | 1..* | CodeableConcept | Care Plan category code describes the type of care plan. Please see CarePlan.category detail for guidance. Slice: Unordered, Open by pattern:$this Binding: CarePlanCategory (example): Identifies what "kind" of plan this is to support differentiation between multiple co-existing plans; e.g. "Home health", "psychiatric", "asthma", "disease management", etc. | ||||
| SΣ | 1..1 | CodeableConcept | (USCDI) Type of plan Binding: CarePlanCategory (example): Identifies what "kind" of plan this is to support differentiation between multiple co-existing plans; e.g. "Home health", "psychiatric", "asthma", "disease management", etc. Required Pattern: At least the following | ||||
 | 0..1 | string | Unique id for inter-element referencing | |||||
| 0..* | Extension | Additional content defined by implementations | |||||
 | 1..* | Coding | Code defined by a terminology system Fixed Value: (complex) | |||||
 | 0..1 | string | Unique id for inter-element referencing | |||||
| 0..* | Extension | Additional content defined by implementations | |||||
| 1..1 | uri | Identity of the terminology system Fixed Value: http://hl7.org/fhir/us/core/CodeSystem/careplan-category | |||||
| 0..1 | string | Version of the system - if relevant | |||||
| 1..1 | code | Symbol in syntax defined by the system Fixed Value: assess-plan | |||||
| 0..1 | string | Representation defined by the system | |||||
| 0..1 | boolean | If this coding was chosen directly by the user | |||||
 | 0..1 | string | Plain text representation of the concept | |||||
| Σ | 0..1 | string | Human-friendly name for the care plan | ||||
| Σ | 0..1 | string | Summary of nature of plan | ||||
| SΣ | 1..1 | Reference(US Core Patient Profile) | (USCDI) Who the care plan is for | ||||
| Σ | 0..1 | Reference(Encounter) | Encounter created as part of | ||||
| Σ | 0..1 | Period | Time period plan covers | ||||
| Σ | 0..1 | dateTime | Date record was first recorded | ||||
| Σ | 0..1 | Reference(Patient | Practitioner | PractitionerRole | Device | RelatedPerson | Organization | CareTeam) | Use the CarePlan custodian extension instead. Use of CarePlan.author is discouraged, it is removed in R5. | ||||
| S | 0..* | Reference(US Core Patient Profile | US Core Practitioner Profile | US Core PractitionerRole Profile | US Core CareTeam Profile | US Core Organization Profile | RelatedPerson | Device | Multiple Chronic Condition Care Plan Care Team) | Who provided the content of the care plan | ||||
| S | 0..* | Reference(Multiple Chronic Condition Care Plan Care Team | US Core CareTeam Profile) | Who's involved in plan? | ||||
| Σ | 0..* | Reference(Condition) | Health issues this plan addresses | ||||
| 0..1 | string | Unique id for inter-element referencing | |||||
| 0..* | Extension | Additional content defined by implementations Slice: Unordered, Open by value:url | |||||
| ΣC | 0..1 | string | Literal reference, Relative, internal or absolute URL | ||||
| Σ | 0..1 | uri | Type the reference refers to (e.g. "Patient") Binding: ResourceType (extensible): Aa resource (or, for logical models, the URI of the logical model). | ||||
| Σ | 0..1 | Identifier | Logical reference, when literal reference is not known | ||||
| Σ | 0..1 | string | Text alternative for the resource | ||||
| S | 0..* | Reference(US Core Blood Pressure Profile | US Core BMI Profile | US Core Body Weight Profile | Multiple Chronic Condition Care Plan Chronic Disease Conditions | Multiple Chronic Condition Care Plan Laboratory Result Observation | Multiple Chronic Condition Care Plan Diagnostic Report and Note | Multiple Chronic Condition Care Plan Procedure | US Core Immunization Profile | Multiple Chronic Condition Care Plan Family History | Document Reference to Patient's Personal Advance Care Plan (Advance Directive) | SDC Questionnaire Response | Multiple Chronic Condition Care Plan Symptom Observation | Multiple Chronic Condition Care Plan Service Request | Multiple Chronic Condition Care Plan Observation SDOH Assessment | Multiple Chronic Condition Care Plan Immunization | Multiple Chronic Condition Care Plan Nutrition Order | Multiple Chronic Condition Care Plan Clinical Impression | Multiple Chronic Condition Care Plan Patient/Caregiver Condition Status Observation | Multiple Chronic Condition Care Plan Questionnaire Response | Multiple Chronic Condition Care Plan Caregiver Considerations Observation | Multiple Chronic Condition Care Plan Clinical Test Observation | US Core RelatedPerson Profile | US Core Observation Occupation Profile) | Please see the libraries of available value sets pertinent for use with the appropriate Multiple Chronic Condition Care Plan Profile for use within the referenced profiles at CarePlan.supportingInfo | ||||
| 0..* | Reference(Multiple Chronic Condition Care Plan Goal) | This Goal represents one or more overarching goal applicable to the entire care plan | |||||
| SC | 0..* | BackboneElement | Action to occur as part of plan. This is the backbone element of the care plan that is the root of care coordination activities. While there can be many activities in a care plan, each activity has only one planned.activityRefence | ||||
| 0..1 | string | Unique id for inter-element referencing | |||||
| 0..* | Extension | Additional content defined by implementations | |||||
| ?!Σ | 0..* | Extension | Extensions that cannot be ignored even if unrecognized | ||||
| 0..* | CodeableConcept | Results of the activity Binding: CarePlanActivityOutcome (example): Identifies the results of the activity. | |||||
| S | 0..* | Reference(Multiple Chronic Condition Care Plan Procedure | Multiple Chronic Condition Care Plan Laboratory Result Observation | US Core Immunization Profile | Multiple Chronic Condition Care Plan Diagnostic Report and Note | US Core Immunization Profile | Multiple Chronic Condition Care Plan Medication Request | Multiple Chronic Condition Care Plan Chronic Disease Conditions | US Core Body Weight Profile | US Core Blood Pressure Profile | Multiple Chronic Condition Care Plan Goal | US Core BMI Profile | Multiple Chronic Condition Care Plan Symptom Observation) | This CarePlan element represents a PERFORMED ACTIVITY. Please see the libraries of available value sets pertinent for use with the appropriate Multiple Chronic Condition Care Plan Profile for use within the referenced profiles at CarePlan.activity.outcomeReference | ||||
| 0..* | Annotation | Comments about the activity status/progress | |||||
| SC | 0..1 | Reference(NutritionOrder | Multiple Chronic Condition Care Plan Medication Request | CommunicationRequest | DeviceRequest | Task | ServiceRequest | VisionPrescription | RequestGroup | Appointment) | This CarePlan element represents a PLANNED ACTIVITY. Please see the libraries of available value sets pertinent for use with the appropriate Multiple Chronic Condition Care Plan Profile for use within the referenced profiles at CarePlan.activity.reference | ||||
| 0..* | Annotation | Comments about the plan | |||||
| Documentation for this format | ||||||||
| Path | Conformance | ValueSet / Code | ||||
| CarePlan.language | preferred | CommonLanguages
| ||||
| CarePlan.text.status | required | NarrativeStatus | ||||
| CarePlan.status | required | RequestStatus | ||||
| CarePlan.intent | required | CarePlanIntent | ||||
| CarePlan.category | example | CarePlanCategory | ||||
| CarePlan.category:AssessPlan | example | Pattern: assess-plan | ||||
| CarePlan.addresses.type | extensible | ResourceType | ||||
| CarePlan.activity.outcomeCodeableConcept | example | CarePlanActivityOutcome | ||||
| CarePlan.activity.detail.kind | required | CarePlanActivityKind | ||||
| CarePlan.activity.detail.code | example | ProcedureCodes(SNOMEDCT) | ||||
| CarePlan.activity.detail.reasonCode | example | SNOMEDCTClinicalFindings | ||||
| CarePlan.activity.detail.status | required | CarePlanActivityStatus | ||||
| CarePlan.activity.detail.product[x] | example | SNOMEDCTMedicationCodes |
| Id | Grade | Path(s) | Details | Requirements |
| cpl-3 | error | CarePlan.activity | Provide a reference or detail, not both : detail.empty() or reference.empty() | |
| ele-1 | error | **ALL** elements | All FHIR elements must have a @value or children : hasValue() or (children().count() > id.count()) | |
| ext-1 | error | **ALL** extensions | Must have either extensions or value[x], not both : extension.exists() != value.exists() | |
| txt-1 | error | CarePlan.text.div | The narrative SHALL contain only the basic html formatting elements and attributes described in chapters 7-11 (except section 4 of chapter 9) and 15 of the HTML 4.0 standard, <a> elements (either name or href), images and internally contained style attributes : htmlChecks() | |
| txt-2 | error | CarePlan.text.div | The narrative SHALL have some non-whitespace content : htmlChecks() |
This structure is derived from USCoreCarePlanProfile
Summary
Must-Support: 9 elements
Prohibited: 1 element
Structures
This structure refers to these other structures:
Extensions
This structure refers to these extensions:
Differential View
This structure is derived from USCoreCarePlanProfile
Key Elements View
| Name | Flags | Card. | Type | Description & Constraints |
|---|---|---|---|---|
| 0..* | USCoreCarePlanProfile | Healthcare plan for patient or group | ||
| ?!Σ | 0..1 | uri | A set of rules under which this content was created |
| S | 0..1 | Narrative | (USCDI) Text summary of the resource, for human interpretation |
| S | 1..1 | code | (USCDI) generated | extensions | additional | empty Binding: US Core Narrative Status (required): Constrained value set of narrative statuses. |
| SC | 1..1 | xhtml | (USCDI) Limited xhtml content |
| 0..1 | Reference(US Core Patient Profile | US Core Practitioner Profile | US Core PractitionerRole Profile | US Core CareTeam Profile | US Core Organization Profile | RelatedPerson | Device | Multiple Chronic Condition Care Plan Care Team) | When populated, the custodian is responsible for the care and maintenance of the care plan. The care plan is attributed to the custodian. The custodian might or might not be a contributor. This CarePlan.custodian extension should be used instead of CarePlan.author which in R4 is currently identified as the designated responsible party and in R5 has been removed. URL: http://hl7.org/fhir/us/mcc/StructureDefinition/custodian | |
| ?! | 0..* | Extension | Extensions that cannot be ignored |
| ?!SΣ | 1..1 | code | (USCDI) draft | active | on-hold | revoked | completed | entered-in-error | unknown Binding: RequestStatus (required): Indicates whether the plan is currently being acted upon, represents future intentions or is now a historical record. |
| ?!SΣ | 1..1 | code | (USCDI) proposal | plan | order | option Binding: CarePlanIntent (required): Codes indicating the degree of authority/intentionality associated with a care plan |
| SΣ | 1..* | CodeableConcept | Care Plan category code describes the type of care plan. Please see CarePlan.category detail for guidance. Slice: Unordered, Open by pattern:$this Binding: CarePlanCategory (example): Identifies what "kind" of plan this is to support differentiation between multiple co-existing plans; e.g. "Home health", "psychiatric", "asthma", "disease management", etc. |
| SΣ | 1..1 | CodeableConcept | (USCDI) Type of plan Binding: CarePlanCategory (example): Identifies what "kind" of plan this is to support differentiation between multiple co-existing plans; e.g. "Home health", "psychiatric", "asthma", "disease management", etc. Required Pattern: At least the following |
| 1..* | Coding | Code defined by a terminology system Fixed Value: (complex) | |
| 1..1 | uri | Identity of the terminology system Fixed Value: http://hl7.org/fhir/us/core/CodeSystem/careplan-category | |
| 1..1 | code | Symbol in syntax defined by the system Fixed Value: assess-plan | |
| SΣ | 1..1 | Reference(US Core Patient Profile) | (USCDI) Who the care plan is for |
| Σ | 0..1 | Reference(Patient | Practitioner | PractitionerRole | Device | RelatedPerson | Organization | CareTeam) | Use the CarePlan custodian extension instead. Use of CarePlan.author is discouraged, it is removed in R5. |
| S | 0..* | Reference(US Core Patient Profile | US Core Practitioner Profile | US Core PractitionerRole Profile | US Core CareTeam Profile | US Core Organization Profile | RelatedPerson | Device | Multiple Chronic Condition Care Plan Care Team) | Who provided the content of the care plan |
| S | 0..* | Reference(Multiple Chronic Condition Care Plan Care Team | US Core CareTeam Profile) | Who's involved in plan? |
| S | 0..* | Reference(US Core Blood Pressure Profile | US Core BMI Profile | US Core Body Weight Profile | Multiple Chronic Condition Care Plan Chronic Disease Conditions | Multiple Chronic Condition Care Plan Laboratory Result Observation | Multiple Chronic Condition Care Plan Diagnostic Report and Note | Multiple Chronic Condition Care Plan Procedure | US Core Immunization Profile | Multiple Chronic Condition Care Plan Family History | Document Reference to Patient's Personal Advance Care Plan (Advance Directive) | SDC Questionnaire Response | Multiple Chronic Condition Care Plan Symptom Observation | Multiple Chronic Condition Care Plan Service Request | Multiple Chronic Condition Care Plan Observation SDOH Assessment | Multiple Chronic Condition Care Plan Immunization | Multiple Chronic Condition Care Plan Nutrition Order | Multiple Chronic Condition Care Plan Clinical Impression | Multiple Chronic Condition Care Plan Patient/Caregiver Condition Status Observation | Multiple Chronic Condition Care Plan Questionnaire Response | Multiple Chronic Condition Care Plan Caregiver Considerations Observation | Multiple Chronic Condition Care Plan Clinical Test Observation | US Core RelatedPerson Profile | US Core Observation Occupation Profile) | Please see the libraries of available value sets pertinent for use with the appropriate Multiple Chronic Condition Care Plan Profile for use within the referenced profiles at CarePlan.supportingInfo |
| 0..* | Reference(Multiple Chronic Condition Care Plan Goal) | This Goal represents one or more overarching goal applicable to the entire care plan | |
| SC | 0..* | BackboneElement | Action to occur as part of plan. This is the backbone element of the care plan that is the root of care coordination activities. While there can be many activities in a care plan, each activity has only one planned.activityRefence |
| ?!Σ | 0..* | Extension | Extensions that cannot be ignored even if unrecognized |
| S | 0..* | Reference(Multiple Chronic Condition Care Plan Procedure | Multiple Chronic Condition Care Plan Laboratory Result Observation | US Core Immunization Profile | Multiple Chronic Condition Care Plan Diagnostic Report and Note | US Core Immunization Profile | Multiple Chronic Condition Care Plan Medication Request | Multiple Chronic Condition Care Plan Chronic Disease Conditions | US Core Body Weight Profile | US Core Blood Pressure Profile | Multiple Chronic Condition Care Plan Goal | US Core BMI Profile | Multiple Chronic Condition Care Plan Symptom Observation) | This CarePlan element represents a PERFORMED ACTIVITY. Please see the libraries of available value sets pertinent for use with the appropriate Multiple Chronic Condition Care Plan Profile for use within the referenced profiles at CarePlan.activity.outcomeReference |
| SC | 0..1 | Reference(NutritionOrder | Multiple Chronic Condition Care Plan Medication Request | CommunicationRequest | DeviceRequest | Task | ServiceRequest | VisionPrescription | RequestGroup | Appointment) | This CarePlan element represents a PLANNED ACTIVITY. Please see the libraries of available value sets pertinent for use with the appropriate Multiple Chronic Condition Care Plan Profile for use within the referenced profiles at CarePlan.activity.reference |
| Documentation for this format | ||||
| Path | Conformance | ValueSet / Code |
| CarePlan.text.status | required | NarrativeStatus |
| CarePlan.status | required | RequestStatus |
| CarePlan.intent | required | CarePlanIntent |
| CarePlan.category | example | CarePlanCategory |
| CarePlan.category:AssessPlan | example | Pattern: assess-plan |
| CarePlan.activity.detail.status | required | CarePlanActivityStatus |
| Id | Grade | Path(s) | Details | Requirements |
| cpl-3 | error | CarePlan.activity | Provide a reference or detail, not both : detail.empty() or reference.empty() | |
| dom-2 | error | CarePlan | If the resource is contained in another resource, it SHALL NOT contain nested Resources : contained.contained.empty() | |
| dom-3 | error | CarePlan | If the resource is contained in another resource, it SHALL be referred to from elsewhere in the resource or SHALL refer to the containing resource : contained.where((('#'+id in (%resource.descendants().reference | %resource.descendants().as(canonical) | %resource.descendants().as(uri) | %resource.descendants().as(url))) or descendants().where(reference = '#').exists() or descendants().where(as(canonical) = '#').exists() or descendants().where(as(canonical) = '#').exists()).not()).trace('unmatched', id).empty() | |
| dom-4 | error | CarePlan | If a resource is contained in another resource, it SHALL NOT have a meta.versionId or a meta.lastUpdated : contained.meta.versionId.empty() and contained.meta.lastUpdated.empty() | |
| dom-5 | error | CarePlan | If a resource is contained in another resource, it SHALL NOT have a security label : contained.meta.security.empty() | |
| dom-6 | best practice | CarePlan | A resource should have narrative for robust management : text.`div`.exists() | |
| ele-1 | error | **ALL** elements | All FHIR elements must have a @value or children : hasValue() or (children().count() > id.count()) | |
| ext-1 | error | **ALL** extensions | Must have either extensions or value[x], not both : extension.exists() != value.exists() | |
| txt-1 | error | CarePlan.text.div | The narrative SHALL contain only the basic html formatting elements and attributes described in chapters 7-11 (except section 4 of chapter 9) and 15 of the HTML 4.0 standard, <a> elements (either name or href), images and internally contained style attributes : htmlChecks() | |
| txt-2 | error | CarePlan.text.div | The narrative SHALL have some non-whitespace content : htmlChecks() |
Snapshot View
| Name | Flags | Card. | Type | Description & Constraints | ||||
|---|---|---|---|---|---|---|---|---|
| 0..* | USCoreCarePlanProfile | Healthcare plan for patient or group | ||||||
| Σ | 0..1 | id | Logical id of this artifact | ||||
| Σ | 0..1 | Meta | Metadata about the resource | ||||
| ?!Σ | 0..1 | uri | A set of rules under which this content was created | ||||
| 0..1 | code | Language of the resource content Binding: CommonLanguages (preferred): A human language.
| |||||
| S | 0..1 | Narrative | (USCDI) Text summary of the resource, for human interpretation | ||||
| 0..1 | string | Unique id for inter-element referencing | |||||
| 0..* | Extension | Additional content defined by implementations Slice: Unordered, Open by value:url | |||||
| S | 1..1 | code | (USCDI) generated | extensions | additional | empty Binding: US Core Narrative Status (required): Constrained value set of narrative statuses. | ||||
| SC | 1..1 | xhtml | (USCDI) Limited xhtml content | ||||
| 0..* | Resource | Contained, inline Resources | |||||
| 0..* | Extension | Extension Slice: Unordered, Open by value:url | |||||
| 0..1 | Reference(US Core Patient Profile | US Core Practitioner Profile | US Core PractitionerRole Profile | US Core CareTeam Profile | US Core Organization Profile | RelatedPerson | Device | Multiple Chronic Condition Care Plan Care Team) | When populated, the custodian is responsible for the care and maintenance of the care plan. The care plan is attributed to the custodian. The custodian might or might not be a contributor. This CarePlan.custodian extension should be used instead of CarePlan.author which in R4 is currently identified as the designated responsible party and in R5 has been removed. URL: http://hl7.org/fhir/us/mcc/StructureDefinition/custodian | |||||
| ?! | 0..* | Extension | Extensions that cannot be ignored | ||||
| Σ | 0..* | Identifier | External Ids for this plan | ||||
| Σ | 0..* | canonical(PlanDefinition | Questionnaire | Measure | ActivityDefinition | OperationDefinition) | Instantiates FHIR protocol or definition | ||||
| Σ | 0..* | uri | Instantiates external protocol or definition | ||||
| Σ | 0..* | Reference(CarePlan) | Fulfills CarePlan | ||||
| Σ | 0..* | Reference(CarePlan) | CarePlan replaced by this CarePlan | ||||
| Σ | 0..* | Reference(CarePlan) | Part of referenced CarePlan | ||||
| ?!SΣ | 1..1 | code | (USCDI) draft | active | on-hold | revoked | completed | entered-in-error | unknown Binding: RequestStatus (required): Indicates whether the plan is currently being acted upon, represents future intentions or is now a historical record. | ||||
| ?!SΣ | 1..1 | code | (USCDI) proposal | plan | order | option Binding: CarePlanIntent (required): Codes indicating the degree of authority/intentionality associated with a care plan | ||||
| SΣ | 1..* | CodeableConcept | Care Plan category code describes the type of care plan. Please see CarePlan.category detail for guidance. Slice: Unordered, Open by pattern:$this Binding: CarePlanCategory (example): Identifies what "kind" of plan this is to support differentiation between multiple co-existing plans; e.g. "Home health", "psychiatric", "asthma", "disease management", etc. | ||||
| SΣ | 1..1 | CodeableConcept | (USCDI) Type of plan Binding: CarePlanCategory (example): Identifies what "kind" of plan this is to support differentiation between multiple co-existing plans; e.g. "Home health", "psychiatric", "asthma", "disease management", etc. Required Pattern: At least the following | ||||
| 0..1 | string | Unique id for inter-element referencing | |||||
| 0..* | Extension | Additional content defined by implementations | |||||
| 1..* | Coding | Code defined by a terminology system Fixed Value: (complex) | |||||
| 0..1 | string | Unique id for inter-element referencing | |||||
| 0..* | Extension | Additional content defined by implementations | |||||
| 1..1 | uri | Identity of the terminology system Fixed Value: http://hl7.org/fhir/us/core/CodeSystem/careplan-category | |||||
| 0..1 | string | Version of the system - if relevant | |||||
| 1..1 | code | Symbol in syntax defined by the system Fixed Value: assess-plan | |||||
| 0..1 | string | Representation defined by the system | |||||
| 0..1 | boolean | If this coding was chosen directly by the user | |||||
| 0..1 | string | Plain text representation of the concept | |||||
| Σ | 0..1 | string | Human-friendly name for the care plan | ||||
| Σ | 0..1 | string | Summary of nature of plan | ||||
| SΣ | 1..1 | Reference(US Core Patient Profile) | (USCDI) Who the care plan is for | ||||
| Σ | 0..1 | Reference(Encounter) | Encounter created as part of | ||||
| Σ | 0..1 | Period | Time period plan covers | ||||
| Σ | 0..1 | dateTime | Date record was first recorded | ||||
| Σ | 0..1 | Reference(Patient | Practitioner | PractitionerRole | Device | RelatedPerson | Organization | CareTeam) | Use the CarePlan custodian extension instead. Use of CarePlan.author is discouraged, it is removed in R5. | ||||
| S | 0..* | Reference(US Core Patient Profile | US Core Practitioner Profile | US Core PractitionerRole Profile | US Core CareTeam Profile | US Core Organization Profile | RelatedPerson | Device | Multiple Chronic Condition Care Plan Care Team) | Who provided the content of the care plan | ||||
| S | 0..* | Reference(Multiple Chronic Condition Care Plan Care Team | US Core CareTeam Profile) | Who's involved in plan? | ||||
| Σ | 0..* | Reference(Condition) | Health issues this plan addresses | ||||
| 0..1 | string | Unique id for inter-element referencing | |||||
| 0..* | Extension | Additional content defined by implementations Slice: Unordered, Open by value:url | |||||
| ΣC | 0..1 | string | Literal reference, Relative, internal or absolute URL | ||||
| Σ | 0..1 | uri | Type the reference refers to (e.g. "Patient") Binding: ResourceType (extensible): Aa resource (or, for logical models, the URI of the logical model). | ||||
| Σ | 0..1 | Identifier | Logical reference, when literal reference is not known | ||||
| Σ | 0..1 | string | Text alternative for the resource | ||||
| S | 0..* | Reference(US Core Blood Pressure Profile | US Core BMI Profile | US Core Body Weight Profile | Multiple Chronic Condition Care Plan Chronic Disease Conditions | Multiple Chronic Condition Care Plan Laboratory Result Observation | Multiple Chronic Condition Care Plan Diagnostic Report and Note | Multiple Chronic Condition Care Plan Procedure | US Core Immunization Profile | Multiple Chronic Condition Care Plan Family History | Document Reference to Patient's Personal Advance Care Plan (Advance Directive) | SDC Questionnaire Response | Multiple Chronic Condition Care Plan Symptom Observation | Multiple Chronic Condition Care Plan Service Request | Multiple Chronic Condition Care Plan Observation SDOH Assessment | Multiple Chronic Condition Care Plan Immunization | Multiple Chronic Condition Care Plan Nutrition Order | Multiple Chronic Condition Care Plan Clinical Impression | Multiple Chronic Condition Care Plan Patient/Caregiver Condition Status Observation | Multiple Chronic Condition Care Plan Questionnaire Response | Multiple Chronic Condition Care Plan Caregiver Considerations Observation | Multiple Chronic Condition Care Plan Clinical Test Observation | US Core RelatedPerson Profile | US Core Observation Occupation Profile) | Please see the libraries of available value sets pertinent for use with the appropriate Multiple Chronic Condition Care Plan Profile for use within the referenced profiles at CarePlan.supportingInfo | ||||
| 0..* | Reference(Multiple Chronic Condition Care Plan Goal) | This Goal represents one or more overarching goal applicable to the entire care plan | |||||
| SC | 0..* | BackboneElement | Action to occur as part of plan. This is the backbone element of the care plan that is the root of care coordination activities. While there can be many activities in a care plan, each activity has only one planned.activityRefence | ||||
| 0..1 | string | Unique id for inter-element referencing | |||||
| 0..* | Extension | Additional content defined by implementations | |||||
| ?!Σ | 0..* | Extension | Extensions that cannot be ignored even if unrecognized | ||||
| 0..* | CodeableConcept | Results of the activity Binding: CarePlanActivityOutcome (example): Identifies the results of the activity. | |||||
| S | 0..* | Reference(Multiple Chronic Condition Care Plan Procedure | Multiple Chronic Condition Care Plan Laboratory Result Observation | US Core Immunization Profile | Multiple Chronic Condition Care Plan Diagnostic Report and Note | US Core Immunization Profile | Multiple Chronic Condition Care Plan Medication Request | Multiple Chronic Condition Care Plan Chronic Disease Conditions | US Core Body Weight Profile | US Core Blood Pressure Profile | Multiple Chronic Condition Care Plan Goal | US Core BMI Profile | Multiple Chronic Condition Care Plan Symptom Observation) | This CarePlan element represents a PERFORMED ACTIVITY. Please see the libraries of available value sets pertinent for use with the appropriate Multiple Chronic Condition Care Plan Profile for use within the referenced profiles at CarePlan.activity.outcomeReference | ||||
| 0..* | Annotation | Comments about the activity status/progress | |||||
| SC | 0..1 | Reference(NutritionOrder | Multiple Chronic Condition Care Plan Medication Request | CommunicationRequest | DeviceRequest | Task | ServiceRequest | VisionPrescription | RequestGroup | Appointment) | This CarePlan element represents a PLANNED ACTIVITY. Please see the libraries of available value sets pertinent for use with the appropriate Multiple Chronic Condition Care Plan Profile for use within the referenced profiles at CarePlan.activity.reference | ||||
| 0..* | Annotation | Comments about the plan | |||||
| Documentation for this format | ||||||||
| Path | Conformance | ValueSet / Code | ||||
| CarePlan.language | preferred | CommonLanguages
| ||||
| CarePlan.text.status | required | NarrativeStatus | ||||
| CarePlan.status | required | RequestStatus | ||||
| CarePlan.intent | required | CarePlanIntent | ||||
| CarePlan.category | example | CarePlanCategory | ||||
| CarePlan.category:AssessPlan | example | Pattern: assess-plan | ||||
| CarePlan.addresses.type | extensible | ResourceType | ||||
| CarePlan.activity.outcomeCodeableConcept | example | CarePlanActivityOutcome | ||||
| CarePlan.activity.detail.kind | required | CarePlanActivityKind | ||||
| CarePlan.activity.detail.code | example | ProcedureCodes(SNOMEDCT) | ||||
| CarePlan.activity.detail.reasonCode | example | SNOMEDCTClinicalFindings | ||||
| CarePlan.activity.detail.status | required | CarePlanActivityStatus | ||||
| CarePlan.activity.detail.product[x] | example | SNOMEDCTMedicationCodes |
| Id | Grade | Path(s) | Details | Requirements |
| cpl-3 | error | CarePlan.activity | Provide a reference or detail, not both : detail.empty() or reference.empty() | |
| ele-1 | error | **ALL** elements | All FHIR elements must have a @value or children : hasValue() or (children().count() > id.count()) | |
| ext-1 | error | **ALL** extensions | Must have either extensions or value[x], not both : extension.exists() != value.exists() | |
| txt-1 | error | CarePlan.text.div | The narrative SHALL contain only the basic html formatting elements and attributes described in chapters 7-11 (except section 4 of chapter 9) and 15 of the HTML 4.0 standard, <a> elements (either name or href), images and internally contained style attributes : htmlChecks() | |
| txt-2 | error | CarePlan.text.div | The narrative SHALL have some non-whitespace content : htmlChecks() |
This structure is derived from USCoreCarePlanProfile
Summary
Must-Support: 9 elements
Prohibited: 1 element
Structures
This structure refers to these other structures:
Extensions
This structure refers to these extensions:
Other representations of profile: CSV, Excel, Schematron
IG © 2020+ HL7 International - Patient Care WG. Package hl7.fhir.us.mcc#1.0.0-ballot2 based on FHIR 4.0.1. Generated 2023-07-28
Links: Table of Contents |
QA Report
| Version History |
 |
Propose a change
|
Propose a change