
This page is part of the FHIR Specification (v0.06: DSTU 1 Ballot 2). The current version which supercedes this version is 5.0.0. For a full list of available versions, see the Directory of published versions
Status: Approved infrastructure resource. Draft for comment
A documentation of healthcare-related information that is assembled together into a single statement of meaning that establishes its own context. A document is composed of a set of resources that include both human and computer readable portions. A human may attest to the accuracy of the human readable portion, and may authenticate and/or sign the entire whole. A document may be kept as a set of logically linked resources, or they may be bundled together in an atom feed.
FHIR resources can be used to build clinical documents that capture information about clinical observations and services. A clinical document is a bundle (a list of resources in an atom feed) that is fixed in scope, frozen in time and authored and/or attested as a set of logically contained resources by humans, organisations and devices. Documents built in this fashion may be exchanged between systems and also persisted in document storage and management systems, including systems such as IHE XDS. Applications claiming conformance to this framework claim to be conformant to "FHIR documents".
All documents have the same structure: a bundle that has a Document resource (see below) first, followed by a series of other resources referenced from the Document header which provides guidance on how they fit together. The bundle gathers all the content of the document into a single XML document which may be signed and managed as required. The resources include both human and computer readable portions.
The document resource identifies the document and its purpose, sets the context of the document and carries key information such as the subject and author. It also divides the document up into a series of sections that contain other resources identified in this specification that carry the content. Any resource referenced directly in the Document resource must be included in the bundle when the document is assembled. Other resources that these referenced resources refer to may also be included in the bundle if the document originator chooses to.
Document profiles can make additional rules about which resources must be included in the bundle along with the resources that are directly referenced in the Document resource. In addition, Document Profiles can specify what sections a document contains and what the constraints on their contents are. Applications should consider publishing conformance statements that identify particular documents they support.
There are two RESTful end-points used for Documents:
Note: While these end-points are defined for use with document resources and document bundles, it is not necessary to use them. Documents may be transferred between systems by using the MailBox target, or by using any other method desired.
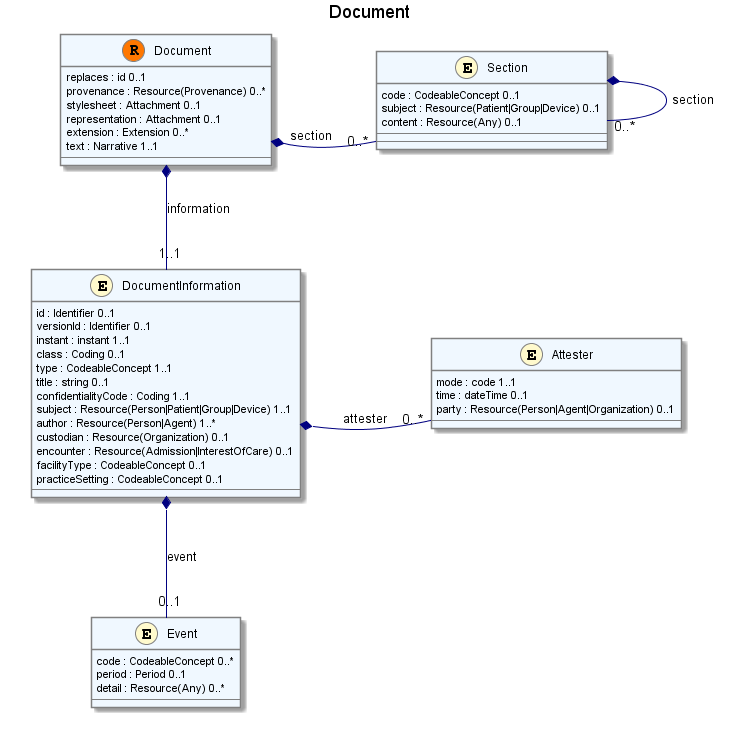
<Document xmlns="http://hl7.org/fhir"> <information> <!-- 1..1 Metadata and context for this document --> <id><!-- 0..1 Identifier logical identifier for document (version-independent) --></id> <versionId><!-- 0..1 Identifier version-specific identifier for document --></versionId> <instant><!-- 1..1 instant Document Creation Time --></instant> <class><!-- 0..1 Coding particular kind of document --></class> <type><!-- 1..1 CodeableConcept Kind of Document (LOINC if possible) --></type> <title><!-- 0..1 string Document Title --></title> <confidentialityCode><!-- 1..1 Coding as defined by Affinity Domain --></confidentialityCode> <subject><!-- 1..1 Resource(Person|Patient|Group|Device) Who/what the document is about --></subject> <author><!-- 1..* Resource(Person|Agent) Who/what authored the final document --></author> <attester> <!-- 0..* Attests to accuracy of document --> <mode><!-- 1..1 code Personal | professional | legal | official --></mode> <time><!-- 0..1 dateTime When document attested --></time> <party><!-- 0..1 Resource(Person|Agent|Organization) Who attested the document --></party> </attester> <custodian><!-- 0..1 Resource(Organization) Org which maintains the document --></custodian> <event> <!-- 0..1 The clinical event/act/item being documented --> <code><!-- 0..* CodeableConcept code(s) that apply to the event being documented --></code> <period><!-- 0..1 Period The period covered by the document --></period> <detail><!-- 0..* Resource(Any) Full details for the event(s) the document concents --></detail> </event> <encounter><!-- 0..1 Resource(Admission|InterestOfCare) Context of the document --></encounter> <facilityType><!-- 0..1 CodeableConcept type of organizational setting --></facilityType> <practiceSetting><!-- 0..1 CodeableConcept clinical speciality of the act --></practiceSetting> </information> <replaces><!-- 0..1 id If this document replaces another --></replaces> <provenance><!-- 0..* Resource(Provenance) Additional provenance about the document and it's parts --></provenance> <stylesheet><!-- 0..1 Attachment Stylesheet to use when rendering the document --></stylesheet> <representation><!-- 0..1 Attachment Alternative representation of the document --></representation> <section> <!-- 0..* Document is broken into sections --> <code><!-- 0..1 CodeableConcept Classification of section (recommended) --></code> <subject><!-- 0..1 Resource(Patient|Group|Device) If section different to document --></subject> <content><!-- 0..1 Resource(Any) The actual data for the section --></content> <section><!-- 0..* Content as for Document.Section Nested Section --></section> </section> <extension><!-- 0..* Extension See Extensions --></extension> <text><!-- 1..1 Narrative Text summary of resource (for human interpretation) --></text> </Document>
Alternate definitions: Schema/Schematron, RDF (to do), XML, XMI (to do), Resource Profile
Terminology Bindings
| Path | Details | Strength |
|---|---|---|
| Document.information.type | LOINC Document Types | complete/preferred |
| Document.information.attester.mode | The way in which a person authenticated a document (see http://hl7.org/fhir/document-attestation-mode for values) | complete/required |
| Document.section.code | LOINC Section Types | complete/preferred |
Constraints
There are two identifiers on the document information: id and versionId. These allow either a logical document id or a version specific id to be provided, or both. This supports multiple different identification strategies. The following combinations are allowed:
Any other combinations do not globally uniquely identity a document, and are therefore not allowed.
Note that there is an additional identifier - the bundle identifier itself (atom feed.id). This must be an absolute URI, and in effect globally unique, but has no other particular meaning anywhere else in the specification. For a document, it can be populated with some URI that is extracted from the versionId or id above, or it can be a new UUID that has no other associated use. Implementers should not rely on its value matching one of the formal document identification elements.
The human display of the Document is the collated narrative portions of following resources (in order):
The document narrative should summarize the important parts of the document header that are required to establish clinical context for the document (other than the subject, which is displayed in its own right). To actually build the combined narrative, simply append all the narrative <div> fragments.
In addition to the basic style rules, which must be followed, a document can contain a style sheet that contains additional styles that apply to the collated narrative. Unless otherwise agreed in local trading partner agreements, applications displaying the collated narrative should use the style sheet provided in the document. Parties entering into such a trading agreement should consider the implications it will have on their long term scope for document exchange very carefully.
The authors and users of Clinical Documents, whether human or software, have obligations that they must satisfy.
A document author is an application that creates a document resource. The author may create new content resources and/or assemble already existing content resources while doing so. A document author has the following responsibilities:
A document user is an application that receives or presents documents, or extracts data from them, or makes decisions because of them. The documents may be received directly from a document author or accessed via a document management system. The document user is responsible for ensuring that received documents are processed and/or rendered in accordance to this specification. A document recipient has the following obligations:
Search Parameters for RESTful searches. The standard parameters also apply. See Searching for more information.
| $page : integer | Starting offset of the first record to return in the search set | single |
| $count : integer | Number of return records requested. The server is not bound to conform | single |
| $id : token | The logical resource id associated with the resource (must be supported by all servers) | single |
| type : qtoken | the type of the document | union |
| date : date | date equal to the document creation time | single |
| date-before : date | date before or equal to the document creation time | single |
| date-after : date | date after or equal to the document creation time | single |
| subject : qtoken | subject of the document | union |
| author : qtoken | author of the document | union |
| attester : qtoken | attester of the document | union |
| context : qtoken | context of the document | union |
| section-type : qtoken | code of the document | union |
| section-content : qtoken | content resource of the section | union |
(See Searching).
 This is an old version of FHIR retained for archive purposes. Do not use for anything else
This is an old version of FHIR retained for archive purposes. Do not use for anything else
Implementers are welcome to experiment with the content defined here, but should note that the contents are subject to change without prior notice.
© HL7.org 2011 - 2012. FHIR v0.06 generated on Tue, Dec 4, 2012 00:04+1100. License