
US Core Implementation Guide
4.0.0 - STU4 Release
US Core Implementation Guide
4.0.0 - STU4 Release
This page is part of the US Core (v4.0.0: STU4) based on FHIR (HL7® FHIR® Standard) R4. The current version which supersedes this version is 8.0.0. For a full list of available versions, see the Directory of published versions. Page versions: R7 R6 R5 R4 R3
The US Core FHIR profiles are designed to be the base set of requirements for FHIR implementation in the US. All US Realm implementation guides SHALL use the US Core profiles or SHALL explicitly state why they are unable to use. Throughout the development of US Core, implementers, government, and clinical community have brought forward additional requirements for US Core. This section outlines the approach to growth, and is holding place for items that with additional profiling and testing will be added to US Core.
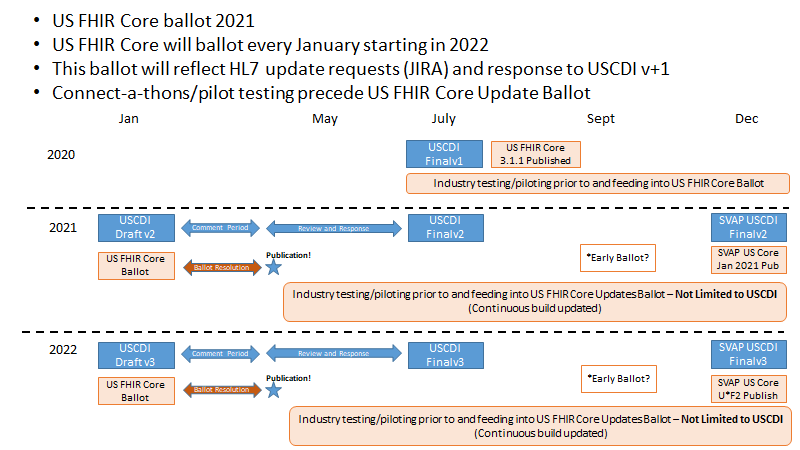
Yearly US Core updates reflect changes to U.S. Core Data for Interoperability (USCDI) v1 and requests from the US Realm FHIR community. This Approach is outlined in the figure below:
The US Core implementation Guide will grow following these steps:
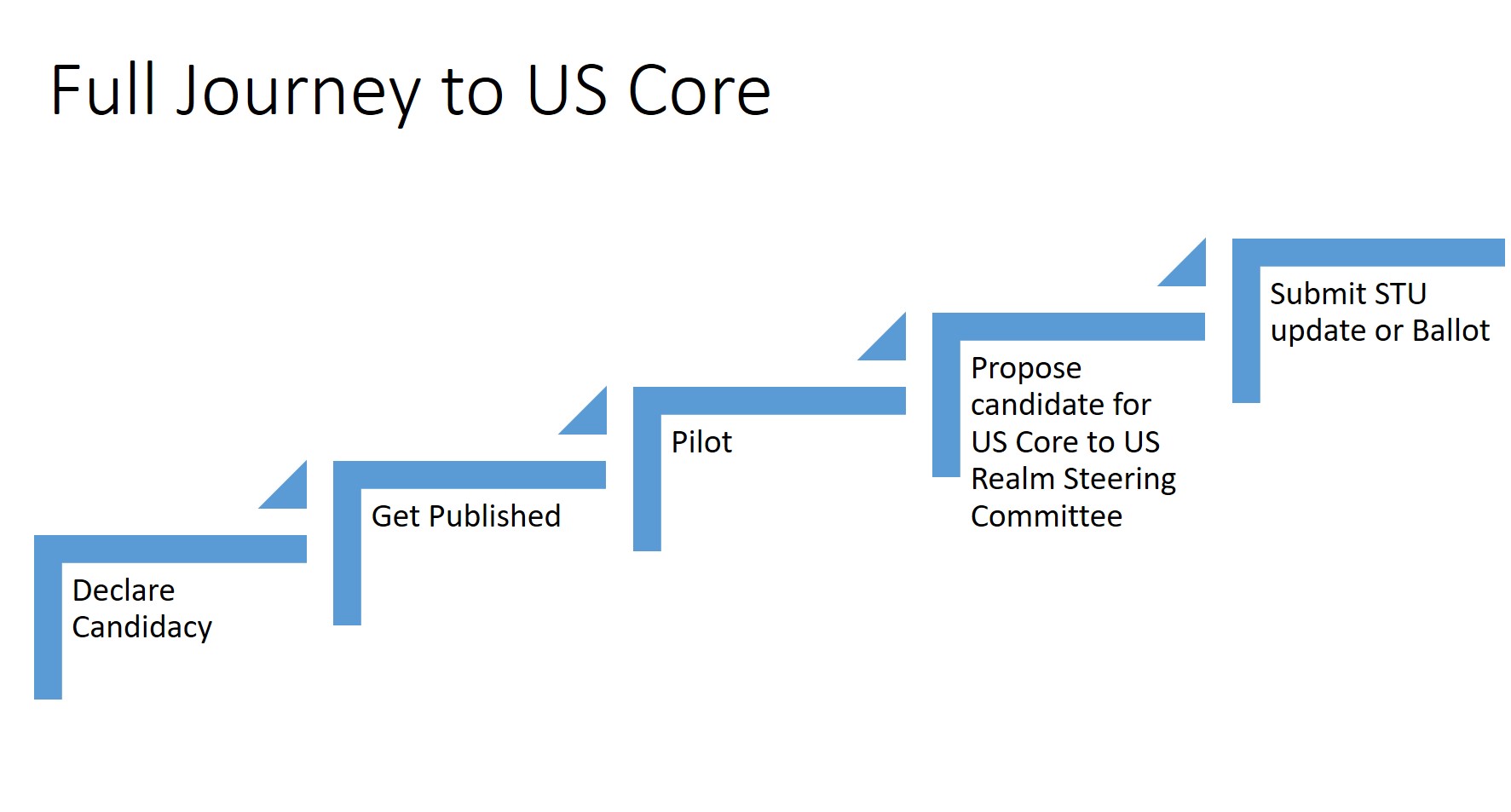
A new US Regulatory requirement may jump over some of these steps, however, regulators should be discouraged from skipping pilot testing. Without pilot testing it’s difficult to understand how a change will affect real-world implementation.
The following items were submitted during a US Core ballot, Argonaut review and testing, and STU comment for consideration to add to us core. Additional requirements gathering is required before testing may occur on these items:
A timezone is a geographical region in which residents observe the same standard time. A time offset is an amount of time subtracted from or added to Coordinated Universal Time (UTC) time to get the current civil time, whether it is standard time or daylight saving time (DST).1
Common practice is to preserve the source data time offsets either as the original offset or converted to Coordinated Universal Time (UTC) time. Making this a requirement is one consideration. Another consideration is the addition of server best practices for preserving source timezones using the FHIR standard timezone extension. A third consideration is providing a client algorithm for resolving time offsets and timezones.
Writing and Updating - Very little guidance is provided on writing and updating data in the context of US Core profiles. There are multiple issues that will need to be considered when defining expected behavior by the various actors to support updates and writes to the data including:
Footnotes
https://en.wikipedia.org/w/index.php?title=UTC_offset#Time_zones_and_time_offsets ↩
IG © 2021+ HL7 International - US Realm Steering Committee. Package hl7.fhir.us.core#4.0.0 based on FHIR 4.0.1. Generated 2021-06-28
Links: Table of Contents |
QA Report
| Version History |
Search |
 |
Propose a change
|
Propose a change