This page is part of the Clinical Guidelines (v2.0.0: STU2) based on FHIR (HL7® FHIR® Standard) R4. This is the current published version in its permanent home (it will always be available at this URL). For a full list of available versions, see the Directory of published versions
Plain Language Summary Goes Here
CPG Home
Official URL: http://hl7.org/fhir/uv/cpg/ImplementationGuide/hl7.fhir.uv.cpg
Version:
2.0.0
Active
as of 2024-11-26
Computable Name: CPG
Other Identifiers: OID:2.16.840.1.113883.4.642.40.48
The FHIR Clinical Guidelines Implementation Guide (CPG IG) provides a means of creating a computable representation of a narrative clinical guideline that is faithful to guideline intent and supports the derivation of downstream capabilities such as cognitive and decision support, quality measures, case reporting, and documentation templates that direct clinical documentation in support of determining guideline compliance.
This implementation guide is organized into the following sections, accessible via the menu bar at the top of every page:
Home: The home page provides summary, introductory, and background information
Approach: The approach page documents the overall approach to representing computable guideline content
Methodology: Describes methodologies for developing computable guideline content
Profiles: Describes expectations for use and an index of the profiles and extensions used in representing computable guideline content
Terminology: Describes expectations for the use of terminology as part of computable guideline content
Libraries: Describes expectations for the use of libraries of computable expressions (e.g. CQL) as part of computable guideline content
Glossary: Glossary of key terms used in the specification
Version History: Index of all versions of this implementation guide
Introduction
This Implementation Guide (IG) supports the development of standards-based computable representations of the content of clinical care guidelines. Its content pertains to technical aspects of digital guidelines implementation and is intended to be usable across multiple use cases across clinical domains as well as in the International Realm.
This IG has been developed through multi-organizational and multidisciplinary efforts (Adapting Clinical Guidelines for the Digital Age, SMART Guidelines, holistically involving a range of stakeholders, including those who work at the beginning of the process (e.g., guideline developers) to the end users (e.g., clinical implementation team representatives, health IT developers, patients/patient advocates), and others in between (e.g., informaticists, communicators, evaluators, public health organizations, clinical quality measure and clinical decision support developers).
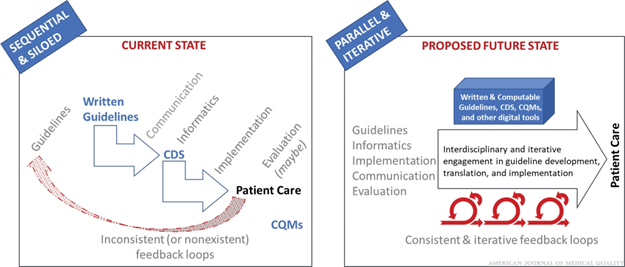
The premise involves determining the representation of clinical practice guideline recommendations in FHIR as part of a parallel and iterative guideline development and implementation process rather than a traditional sequential and siloed process (Figure 1.1). By including all the relevant perspectives (e.g., guideline authors, informaticists, implementers, communicators, evaluators) as part of the iterative process, the resulting computable representation of the recommendations should be well-vetted and more readily implemented across multiple clinical domains.
Figure 1.1 High-level current state (siloed and sequential) and proposed future state (parallel and iterative) process for guideline development and implementation Source.
Scope
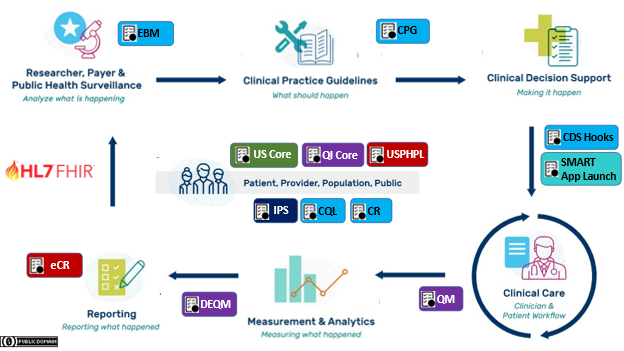
Figure 1.2 Clinical Quality Lifecycle with situated standards to address each respective phase. The CPG-IG addresses a critical gap in explicitly formalizing the guideline recommendations and other guideline features as computer-interpretable for downstream consumption and closing the feedback and feedforward loop(s).
Translating guideline recommendations and other types of guidance into practice has historically been a site-by-site exercise that has been disconnected from guideline/guidance development, creating unnecessary redundancies and introducing potential errors in translation that can lead to inconsistencies in how the guideline or guidance is executed. This clinical practice guidelines implementation guide (CPG-IG) consists of standards and a standardized, scalable approach to help make the effort of translating and implementing clinical practice guidelines and other types of guidance more efficient and effective. Key aspects include:
An integrated guideline/guidance development and implementation process, referred to as "the integrated process" Source
Common standards that can work across the entire clinical quality ecosystem (Figure 1.2) and different electronic health record (EHR) platforms
Closed-loop guideline content and information flow inclusive of feedback and feedforward processes (i.e., high-level "Proposed Future State" in Figure 1.1 and detailed in Figure 1.3)
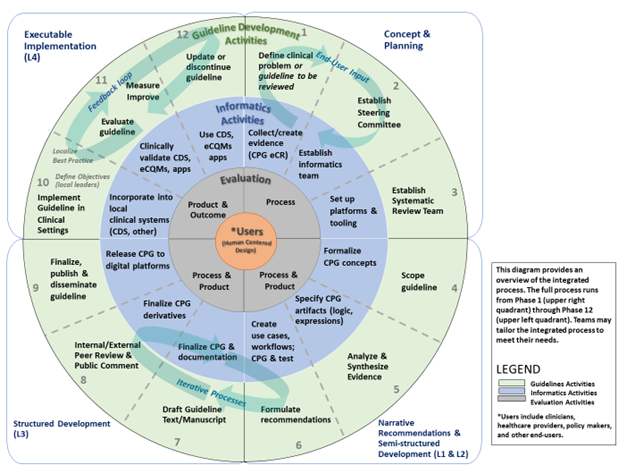
Figure 1.3 The integrated process with integrated evaluation in guideline development and implementation, showing a human-cnetered design approach to co-develop marrative and computable guidelines and build in evaluation, with feedback and feedforward loops throughout the process. (Source and Source).
This IG is focused on the development of computable representations of clinical guideline content as FHIR knowledge artifacts. Since the initial publication, much of the guidance around the content management lifecycle (Shareable, Publishable, Computable, and Executable profile categories) has been generalized to apply across similar content management use cases in other FHIR IGs and is now available in the Canonical Resource Management Infrastructure (CRMI) IG. Content conforming to this CPG IG should make use of the content development approach supported by the CRMI IG.
In addition, the initial publication of this IG included conformance and guidance related to the use of Clinical Quality Language (CQL). This material has been generalized to apply across similar use cases in other FHIR IGs and is now available in the Using CQL With FHIR implementation guide. Content conforming to this CPG IG should make use of the CQL approach supported by the Using CQL With FHIR IG.
Goals
The purpose of the CPG-IG is to:
Enable computable guideline specification to occur concurrently with guideline development;
Faithfully express guideline intent, including rationale and linkage to evidence-base;
Enable efficient and effective use and reuse of the guideline specification in downstream capabilities;
Accelerate the development of computable guideline specifications and interventions through an integrated, cross-functional, rapid-cycle (Agile) development process that is inclusive of local implementation;
More closely tie guideline intent, interventions, and measurements; and
Provide closed-loop (feedback and feedforward loops) across the knowledge, practice, and discovery or evidence ecosystems.
Direct goals:
Reduce duplicate development effort involved in the implementation of clinical practice guideline recommendations in clinical systems
Reduce unnecessary and/or unintentional variability in clinical practice guideline implementation
Improve efficiency and effectiveness of guideline dissemination and implementation processes (e.g. decrease time to uptake of clinical best practices)
Measure compliance with clinical practice guideline recommendations
Improve appropriate compliance with clinical practice guideline recommendations
Afford means for full lifecycle feedback loop in best practice development process (e.g. Professional Guideline Development, Learning Health System, Clinical Translational and Implementation Sciences) including basic considerations for discovery to delivery.
Complement without duplication EBM, MedMorph, eCR, DEQM, QM, and other related IGs
Indirect goals:
Minimize the time needed to implement clinical practice guideline recommendations in clinical systems
Improve the ability to share computable biomedical knowledge artifacts (clinical knowledge definitions, value sets, order sets, expression logic, interventions, etc.)
Enhance the value of computable guidelines (decrease cost/effort, increase utility/usability)
The primary objective of the CPG approach to codifying clinical practice guidelines is to accelerate the translation and delivery of evidence-based and best practice recommendations to the point of care. The CPG-IG was developed through multi-stakeholder engagement (e.g., guideline developers, knowledge engineers, clinical implementers, standards experts, patient and caregiver advocates, governmental and nongovernmental agencies, and others) to evolve the development approach and means of expressing clinical practice guidelines in computable formats. These stakeholders identified the need to concurrently and iteratively develop computable formats along with the narrative guidelines/guidance. As such, the knowledge engineering process, inclusive of elicitation, translation, specification, and formal representation, must be integrated with the guideline development process and serve the function of translating between the clinical domain and the formal, computable expressions thereof. The Approach section describes some of the fundamentals of these activities as well as the concept, means, and performances to carry out this activity.
Secondarily, we describe how these activities interact with adjacent and related activities as well as content and related standards in the broader knowledge ecosystem (inclusive of evidence ecosystem, guideline developers, guideline-directed care, quality measure ecosystem, registry community, etc.). This includes upstream activities, such as evidence generation and knowledge discovery, and downstream activities, such as patient care, decision support (i.e., CDS), and advanced cognitive support (e.g., providing options within the clinical workflow that offer evidence-based, patient-centered information to support clinical judgement), quality measurement and reporting, and electronic case reporting (for similarly scoped conditions). All can serve to inform subsequent iterations of clinical guidelines and guideline-directed care and thus have a key role in the learning health system.
Audience
This IG provides both an approach and suggested methodology for computable representation of clinical practice guidelines, so the audience for this guide is broad and inclusive of an array of roles across the spectrum of clinical guideline development and implementation, from clinical guideline developers and authors, through clinical informaticists, health system integrators and clinical systems developers. Areas of the IG that are more technical assume familiarity with relevant standards, including FHIR and CQL, though links are provided to reference materials for further reading.
The CPG Approach section highlights:
Various highly specialized and technical participants in the “Knowledge-to-Delivery-to-Discovery” ecosystem that often interact with each other’s work products but may not interact directly with each other;
How the HL7 CPG-IG recognizes the technical participants' distinct and valuable work and provides numerous opportunities to reuse domain standards (e.g., FHIR and other HL7 IG's); and
A reconceptualization of work processes that share and reuse essential information and content.
Much of this work has been informed by several international efforts, including the U.S. Centers for Disease Control and Prevention’s (CDC’s) Adapting Clinical Guidelines for the Digital Age initiative (ref), the World Health Organization’s (WHO’s) Antenatal Care Guidelines (ref), the HL7 Clinical Decision Support and Clinical Quality Information Working Groups, and numerous other publicly funded and private sector initiatives, including local health system implementations of guidelines and in-workflow pathways.
Notes to Target Audiences:
To the Guideline Developer: Working in parallel with knowledge engineers and other downstream consumers (e.g., local implementers) can identify areas within the guideline that need clarification, helping improve the narrative, provide opportunity to review the translation of the tools for fidelity to the guideline, and get early feedback from end-consumers of the guideline work product – all before the guidelines or tools are published. These adjustments should not change the intent of the guideline but rather should make the intended recommendations more implementable.
To the Knowledge Engineer: Working in parallel with guideline developers allows validation of translations directly with the “source of truth,” helping ensure accuracy. Working in parallel with downstream consumers (e.g., local implementers) provides the ability to confirm feasibility and validity for the users of the artifacts as they are produced by knowledge engineers and may even provide a useful means to build and validate once (i.e., without unnecessary redundancy) against real-world data and implementations.
To the Downstream Consumers: Being involved with the guideline development and knowledge engineering can help identify issues early in the process and optimize incorporation of the knowledge into downstream products that aid in implementation, such as apps, measures, or other point-of-care tools, and significantly reduce the rework of re-engineering parts of the guideline locally, ultimately saving time and effort.
To the Local Implementer: The main goal of the knowledge developed is to implement it in practice. Having local implementers (both clinicians and informaticians) involved with guideline development and knowledge engineering allows for the ability to communicate anticipated issues for implementation so that guideline developers or knowledge engineers have the opportunity to adjust their respective products in order to help optimize the ease and positive impact of implementation. These adjustments should not change the intent of the guideline but rather should make the intended reommendations more implementable. A computable guideline representation can significantly reduce rework, saving time and effort for local implementations.
To the Evidence Ecosystem: Taking a holistic approach to guideline development and implementation includes considerations for learning and continuous improvement through feedback and feedforward loops. A number of activities in the knowledge ecosystem that serve specific functions (e.g., case reporting to public health, quality reporting to payers, quality/data reporting to medical society registries, etc.) could also help provide the evidence that can inform updates to the guidelines/guidance. This evidence may be based on patient-level, point-of-care guideline usage, and detailed tracking thereof, affording new means of collecting evidence.
Using approaches, standards, and techniques addressed in further detail in individual sections, this CPG IG can serve a critical role in the virtuous cycle of a Learning Health System.
Background
The need for computable care guidelines can be considered in the context of the data lifecycle, where the representation of the guideline recommendations in FHIR helps deliver actionable knowledge. By translating the recommendations in clinical practice guidelines at the source, and disseminating a computable version along with the narrative version of the guidelines, the effort of translation need not be repeated across every organization that intends to apply the recommendations. Likewise, unnecessary or unintentional variations as a result of duplicative translation efforts could be prevented with a standard, computable version that is ready to be implemented. In removing the need for translating recommendations at each local clinical system, and removing as much variation as possible through a standard translation, the time needed to apply the recommendations in practice should also be reduced, helping scientific evidence reach patient care more easily, quickly, accurately, and consistently.
In considering common patterns across multiple guidelines, this implementation guide can apply to a variety of use cases across multiple clinical domains, as is evidenced by the examples provided. These common patterns not only create a way to organize the content for the translation into computable recommendations but also help implementers operationalize the recommendations within clinical workflows.
In particular, the translation into tools like CDS and eCQMs applies common health IT standards like Fast Healthcare Interoperability Resources (FHIR) and Clinical Quality Language (CQL). How to use these standards to develop shareable, platform-independent tools based on guidelines/guidance for a variety of diseases, conditions, or preventive care is the primary focus of this CPG-IG, including this Approach section. Secondarily, this CPG-IG shows how using FHIR can help with other data-focused activities, such as public health reporting (i.e., using electronic case reports) or quality reporting (i.e., using eCQMs), that provide a feedback loop that feeds the evidence. The evidence can also be represented using FHIR (i.e., EBM-on-FHIR) and could be applied in summarizing evidence and updating guidelines/guidance. This completes the "data lifecycle" that allows for continuous learning and improvement – a "learning health system". The CPG-IG approach can be a key component of a learning health system in times requiring rapid response, where knowledge of best practice is not well-known.
It is important to note that this effort is a concerted attempt to build on, learn from, contribute to, and work with existing approaches, initiatives, and efforts in guideline development, translation, and implementation. The contribution of this implementation guide is focused on describing a best-practices conceptual approach combined with a practical methodology that leverages the interoperability framework provided by FHIR as a way to overcome the impedance mismatch between knowledge and clinical data models that is commonly encountered by efforts in this space. The approach and methodologies presented here are the combined result of many person years of work across multiple initiatives and coordinated with groups like Health eDecisions, Clinical Quality Framework initiative, the CDC's Adapting Clinical Guidelines for the Digital Age intiative, the BPM+ for Health initiative, IHE's Computable Care Guidelines initiative, and the WHO's SMART Guidelines initiative. Feedback on the approach and methodologies are welcomed and encouraged. See the references section for further reading and background that informs the approach taken here.
References
Adapting Clinical Guidelines for the Digital Age – American Journal of Medical Quality - September/October 2023 - Volume 38 – Supplement 2 - https://journals.lww.com/ajmqonline/toc/2023/09002
Adapting Clinical Guidelines for the Digital Age: Summary of a Holistic and Multidisciplinary Approach. American Journal of Medical Quality 38(5S):p S3-S11, September/October 2023. https://doi.org/10.1097/JMQ.0000000000000138
An Integrated Process for Co-Developing and Implementing Written and Computable Clinical Practice Guidelines. American Journal of Medical Quality 38(5S):p S12-S34, September/October 2023. https://doi.org/10.1097/JMQ.0000000000000137
An Evaluation Framework for a Novel Process to Codevelop Written and Computable Guidelines. American Journal of Medical Quality 38(5S):p S35-S45, September/October 2023. https://doi.org/10.1097/JMQ.0000000000000140
Adapted Kaizen: Multi-Organizational Complex Process Redesign for Adapting Clinical Guidelines for the Digital Age. American Journal of Medical Quality 38(5S):p S46-S59, September/October 2023. https://doi.org/10.1097/JMQ.0000000000000133
WHO SMART guidelines: optimising country-level use of guideline recommendations in the digital age. Lancet Digit Health. 2021 Apr;3(4):e213-e216. https://doi.org/10.1016/S2589-7500(21)00038-8
Experiences in aligning WHO SMART guidelines to classification and terminology standards. BMJ Health Care Inform. 2023 Aug;30(1):e100691. https://doi.org/10.1136/bmjhci-2022-100691
A multi-layered framework for disseminating knowledge for computer-based decision support. Journal of the American Medical Informatics Association 2011 Dec; 18(Suppl 1): i132-i139. https://doi.org/10.1136/amiajnl-2011-000334
An Ontological Framework for Adaptive Medical Workflow. Journal of Biomedical Informatics Volume 41, Issue 5, October 2008, Pages 829-836. https://doi.org/10.1016/j.jbi.2008.05.012
Comparing Computer-interpretable Guideline Models: A Case-study Approach. Journal of the American Medical Informatics Association Volume 10, Issue 1, January 2003, Pages 52–68. https://doi.org/10.1197/jamia.M1135
Computer-interpretable clinical guidelines: A methodological review. Journal of Biomedical Informatics Volume 46, Issue 4, August 2013, Pages 744-763. https://doi.org/10.1016/j.jbi.2013.06.009
Computerization of workflows, guidelines, and care pathways: a review of implementation challenges for process-oriented health information systems. Journal of the American Medical Informatics Association, Volume 18, Issue 6, November 2011, Pages 738–748. https://doi.org/10.1136/amiajnl-2010-000033
Conceptual alignment of electronic health record data with guideline and workflow knowledge. International Journal of Medical Informatics 64 (2001) 259–274. https://doi.org/10.1016/S1386-5056(01)00196-4
GEM: A Proposal for a More Comprehensive Guideline Document Model Using XML. Journal of the American Medical Informatics Association, Volume 7, Issue 5, September 2000, Pages 488–498. https://doi.org/10.1136/jamia.2000.0070488
GLIF3: a representation format for sharable computer-interpretable clinical practice guidelines. Journal of Biomedical Informatics Volume 37, Issue 3, June 2004, Pages 147-161. https://doi.org/10.1016/j.jbi.2004.04.002
Representation primitives, process models and patient data in computer-interpretable clinical practice guidelines: A literature review of guideline representation models. International Journal of Medical Informatics, Volume 68, Issues 1–3, 2002, Pages 59-70, ISSN 1386-5056, https://doi.org/10.1016/S1386-5056(02)00065-5.
Contributor, Co-Chair (Patient Care), IHE Co-Chair (Patient Care Coordination)
Brian Kaney
Vermonster
Editor
James Kariuki
CDC, Health Scientist
Contributor
Kensaku Kawamoto
University of Utah
Contributor, Co-Chair (Clinical Decision Support)
Robert Lario
University of Utah/US Department of Veterans Affairs, Health Standards Architect
Contributor
Taylor Le
Vermonster
Editor
Ira M. Lubin, PhD
CDC, Health Scientist
Contributor
Irene Maitha
Technical Project Manager, Digital Health
Contributor
Laura Haak Marcial
RTI International, Health Informaticist
Contributor
Robert McClure
Contributor, Co-Chair (Vocabulary)
Maria Michaels
AHRQ, Special Expert for Digital Health (formerly CDC, Senior Public Health Advisor)
Editor
Blackford Middleton
Contributor
Anvil D. Nel
LIFELINE TECH (Pty) Ltd.
Contributor
Nikhil Patel
NHS, Physician
Contributor
Bryn Rhodes
Smile Digital Health
Editor, Co-Chair (Clinical Decision Support)
Derek Ritz
ecGroup Inc., Principal Consultant
Contributor, IHE Co-Chair (Quality Reporting and Public Health)
Susan J. Robinson
CDC, Senior Advisor (retired)
Contributor
Julie Scherer
Motive Medical Intelligence, Chief Informatics Officer
Contributor
Julia Skapik
Contributor
Larie Smoyer
Motive Medical Intelligence, VP of Product Development
Contributor
Davide Sottara
Mayo Clinic
Contributor
Keith Toussaint
KMT Strategies, Principal
Contributor
Jodi Wachs
Clinical Informaticist
Contributor
David Winters
The MITRE Corporation
Contributor
Cross Version Analysis
This is an R4 IG. None of the features it uses are changed in R4B, so it can be used as is with R4B systems. Packages for both R4 (hl7.fhir.uv.cpg.r4) and R4B (hl7.fhir.uv.cpg.r4b) are available.
Automatically added as a dependency - all IGs depend on the HL7 Extension Pack
Package hl7.fhir.uv.extensions.r4#5.1.0
This IG defines the global extensions - the ones defined for everyone. These extensions are always in scope wherever FHIR is being used (built Sat, Apr 27, 2024 18:39+1000+10:00)
Globals Table
There are no Global profiles defined
IP Statements
This publication includes IP covered under the following statements.
The UCUM codes, UCUM table (regardless of format), and UCUM Specification are copyright 1999-2009, Regenstrief Institute, Inc. and the Unified Codes for Units of Measures (UCUM) Organization. All rights reserved. https://ucum.org/trac/wiki/TermsOfUse
This material contains content that is copyright of SNOMED International. Implementers of these specifications must have the appropriate SNOMED CT Affiliate license - for more information contact https://www.snomed.org/get-snomed or info@snomed.org.


 Clinical Practice Guidelines
Clinical Practice Guidelines

 |
Propose a change
|
Propose a change