
Clinical Practice Guidelines
2.0.0-ballot - ballot
![]()
Clinical Practice Guidelines
2.0.0-ballot - ballot
![]()
This page is part of the Clinical Guidelines (v2.0.0-ballot: STU2 Ballot 1) based on FHIR (HL7® FHIR® Standard) R4. The current version which supersedes this version is 2.0.0. For a full list of available versions, see the Directory of published versions
The approach taken by this implementation guide is to consider three broad challenges of clinical guideline implementation:
Note that the levels of knowledge representation are a continuum, with discrete categories introduced in the methodology to help inform discussions and communicate the concepts involved. Typically, the initial guideline content is published in narrative form (L1), but guidelines will often contain diagrams, charts, and other depictions that lean towards semi-structured (L2) representation.
This implementation guide utilizes a previously established clinical decision support (CDS) implementation model to move from a narrative clinical guideline to computable content. This model defines four (4) ‘levels’ of knowledge representation:
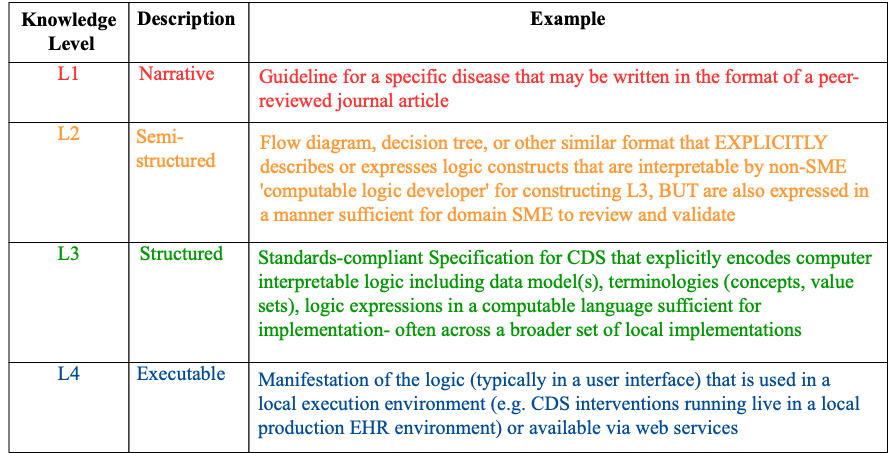
Level 1 (L1) is the clinical guideline in narrative form often in Portable Document Format (PDF), and includes:
Level 2 (L2) is semi-structured and generally consists of process and workflow diagrams, user stories, and personas that provide contextual and descriptive information about the steps involved in each recommendation of the guideline. This level generally includes:
Level 3 (L3) is a computable representation of the content in the guideline and can be shared across health systems and implementation settings. This level is the primary focus of this implementation guide and as such throughout much of this implementation guide when we refer to formalized knowledge assets (or formalisms and expressions) we are almost exclusively referring to this level of representation (computable). They generally consists of:
Level 4 (L4) is executable software running in a clinical system (e.g., EHR, registry, exchange, quality measurement module). This is the local implementation and generally involves:
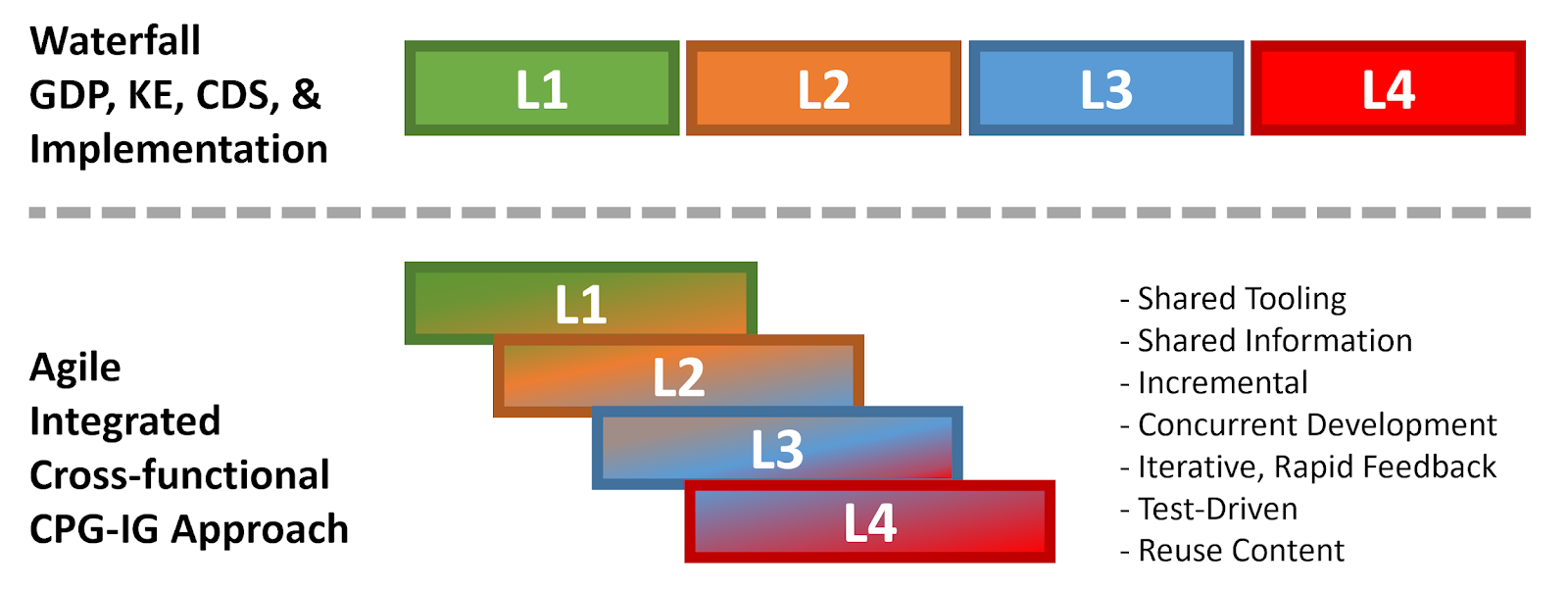
As will be discussed further in the Agile CPG development approach (see section on Knowledge Engineering), these levels of representation may begin to overlap or blur and may not follow an entirely linear or successive progression for sequential development maturation. Furthermore, tooling capabilities may afford translation across levels of representation and some levels may not be entirely expressed as the tools user interface and internal translation capabilities facilitate traversing these levels. This will become more evident and described in more detail in the section on the Agile CPG development approach.
IG © 2023+ HL7 International / Clinical Decision Support. Package hl7.fhir.uv.cpg#2.0.0-ballot based on FHIR 4.0.1. Generated 2023-12-19
Links: Table of Contents |
QA Report
| Version History |
 |
Propose a change
|
Propose a change