
CardX Hypertension Management
1.0.0 - STU1
![]()
CardX Hypertension Management
1.0.0 - STU1
![]()
This page is part of the CardX Hypertension Management IG (v1.0.0: STU1) based on FHIR (HL7® FHIR® Standard) R4. This is the current published version. For a full list of available versions, see the Directory of published versions
Heart disease and stroke are the first and fifth leading causes of death in the U.S. and hypertension is a major risk factor for both. Uncontrolled hypertension can lead to heart attacks, strokes, heart failure, kidney disease, dementia later in life, and other serious clinical sequelae 1. Currently, almost half of adults (48.1%, 119.9M) have hypertension and fewer than one in four has their blood pressure controlled to safe levels (22.5%, 27.0M), defined as <130/80 mmHg in the hypertension management clinical guideline from the American College of Cardiology and the American Heart Association. Non-Hispanic Black persons are less likely to have their blood pressure controlled and more likely to develop hypertension at younger ages than non-Hispanic White persons 2.
Hypertension management is multifaceted and may include antihypertensive medications, lifestyle modifications, and self-measured blood pressure monitoring (SMBP). SMBP, also known as home blood pressure monitoring, is an evidence-based strategy that has been shown to improve medication adherence, reduce therapeutic inertia, and improve blood pressure control. Multiple domestic and international guidelines call for its use in confirming new diagnoses of hypertension and to monitor therapeutic changes until blood pressure control is achieved. Optimal SMBP monitoring includes the remote exchange of patient-generated blood pressure readings to their clinical team who can interpret readings and transmit back titration and/or lifestyle modification advice. Many federal initiatives and national organizations have been working towards widespread implementation of SMBP but barriers exist 3. Lack of interoperable health information technology has been identified as a consistent barrier to SMBP implementation. Interoperability standards are needed to capture and exchange data from patient-generated SMBP readings, the health system, and pertinent data intermediaries.
Sarah Smith, a 54-year-old Black woman with hypertension, had a routine follow-up visit with her primary care provider, Dr. Nolan. Despite being on an antihypertensive medication for two months, Sarah’s blood pressure was elevated in the clinic at 149/92 mmHg. Dr. Nolan recommended adding a second class of antihypertensive medication to her regimen. They discussed the risks of high blood pressure and concerns she had about taking more medication. Ultimately, Sarah agreed that adding another medication to get her blood pressure under control was the right course of action for her.
Dr. Nolan also suggested that Sarah enroll in their clinic’s self-measured blood pressure monitoring (SMBP) program so she could see the impacts of taking her medication or making lifestyle modifications while Dr. Nolan would receive a pattern of her blood pressure readings remotely to monitor the impact of her medication change – without Sarah needing to come back into the office to have her blood pressure checked. Sarah was introduced to the clinic’s SMBP coordinator and digital navigator, Angela, who enrolled her in their program. Sarah was fitted with a properly sized cuff and provided a validated blood pressure device. A list of universally validated blood pressure monitor can be accessed from the Stride BP website. Angela helped Sarah download the blood pressure device’s app, paired her blood pressure device with her phone using Bluetooth, and helped her enter the proper codes allowing the blood pressure reading to be visible by the practice team including her physician. Angela then demonstrated how to properly use the device, trained her on proper preparation and positioning, and provided her with her physician’s protocol with frequency and duration of SMBP. Next, Angela removed the cuff from Sarah’s arm, asked Sarah to demonstrate taking her blood pressure correctly, and confirmed that the blood pressure readings were submitted through the app to a clinical repository (Personal Health Intermediary). Finally, Sarah was given educational materials to reinforce what she had learned.
For the next seven days, Sarah took her blood pressure at home twice in the morning and twice in the evening as instructed. Sarah ensured her phone and the SMBP device were connected via Bluetooth and verified her data were being sent to the app Angela had set up for her. The app on Sarah’s phone was connected to the Personal Health Intermediary which, on a pre-set cadence (for example every seven days from the point of enrollment), sends average blood pressure readings to Sarah’s chart. An average blood pressure is defined as the statistical concept of the mean or average of two or more self-measured blood pressure readings. The average blood pressure has systolic and diastolic components. Angela monitored the EHR, viewed the average blood pressure readings, and notified Dr. Nolan that Sarah’s readings were available for review. Dr. Nolan reviewed Sarah’s SMBP average and let her know the new medication was working; she should continue taking it as prescribed and continue making the lifestyle modifications they discussed. He also asked her to continue taking her blood pressure at home and scheduled a follow-up telehealth visit with Sarah within four weeks. He instructed Sarah to reach out to Angela if she has any questions or concerns or use the patient portal to send Dr. Nolan a message.
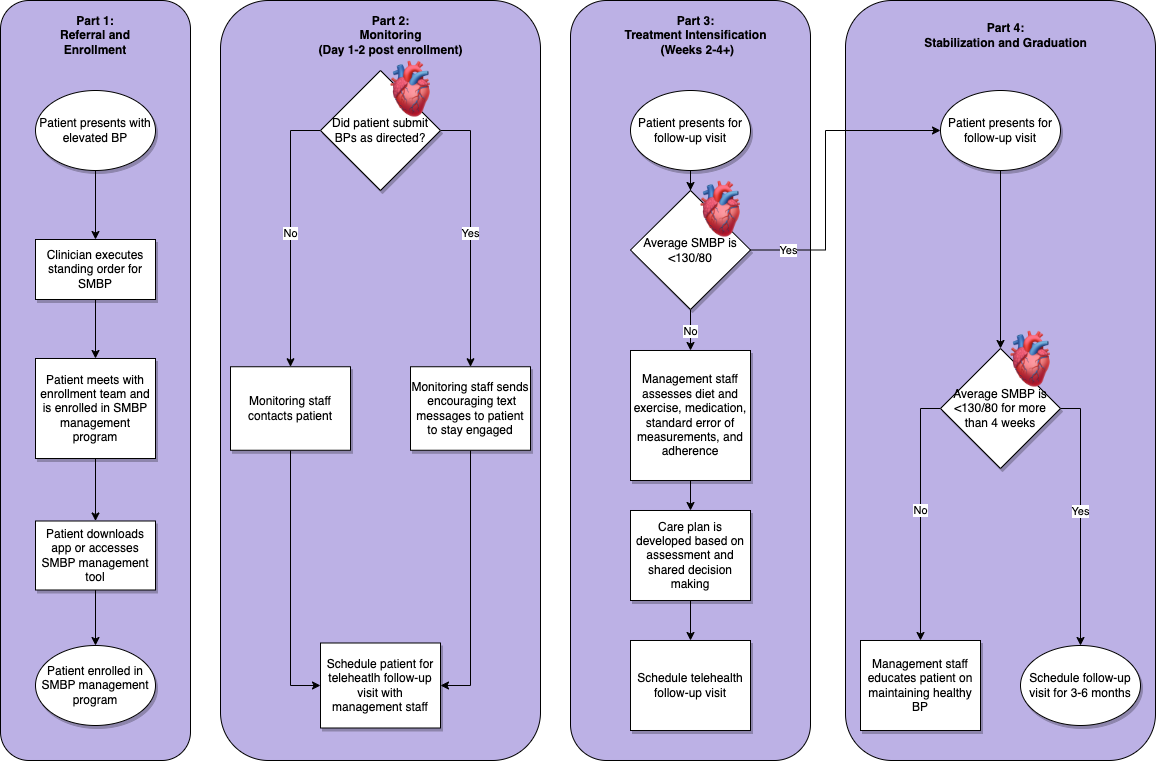
The following diagram developed by the CDC Million Hearts, provides an overview of the typical clinical workflow for a patient enrolled in an SMBP program. The processes in this diagram can be useful when understanding how and when clinical information is exchanged from the patient to the clinician. The Technical Scenarios page provides an in-depth description of how the profiles defined in the IG support this workflow.
ACCF/AHA 2011 key data elements and definitions of a base cardiovascular vocabulary for electronic health records: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Clinical Data Standards
ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ASH/ASPC/NMA/PCNA Guideline for the Prevention, Detection, Evaluation, and Management of High Blood Pressure in Adults: Executive Summary: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines
Cumulative Incidence of Hypertension by 55 Years of Age in Blacks and Whites: The CARDIA Study ↩
Guideline for the Prevention, Detection, Evaluation, and Management of High Blood Pressure in Adults: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines ↩
IG © 2022+ HL7 International / Clinical Interoperability Council. Package hl7.fhir.uv.cardx-htn-mng#1.0.0 based on FHIR 4.0.1. Generated 2024-12-12
Links: Table of Contents |
QA Report
| Version History |
 |
Propose a change
|
Propose a change