
PACIO Personal Functioning and Engagement Implementation Guide
1.0.0-ballot - ballot1
US
PACIO Personal Functioning and Engagement Implementation Guide
1.0.0-ballot - ballot1
US
This page is part of the PACIO Personal Functioning and Engagement Implementation Guide (v1.0.0-ballot: STU 1 Ballot 1) based on FHIR (HL7® FHIR® Standard) R4. The current version which supersedes this version is 2.0.0. For a full list of available versions, see the Directory of published versions
The Personal Functioning and Engagement IG defines the data structures for exchanging information related to an individual’s functioning, both in term of their body as well as their activities and participation in society. This includes observation data (characteristics that can be tested, measured, or observed and are communicated with a name-value pair structure) as well as related clinical care.
The following scenario illustrates one situation in which this IG enables sharing of important information across many care settings, focusing on long-term post-acute care (LTPAC) and health domains of interest in that setting such as mobility, self care, mental functions, and communication.
Post-actute care (PAC) providers and caregivers are particulary interested the functioning and engagement of their patients. PAC supports the recovery and rehabilitation of individuals and aims to enable them to live and act as independently as possible. To identify necessary interventions and track progress, PAC providers, caregivers, and payers collect and document observational data on the patient’s abilities and interactions. However, as the following scenario shows, they interact with many other healthcare settings and both rely on them for information on a patient’s functioning and can provide valuable information that informs ongoing care. Figure 1 illustrates a common scenario for an elderly patient, Betsy Smith, moving through the healthcare ecosystem.
The journey starts with Betsy in her home. She has a medical event that results in an emergency medical service (EMS) transport to Hospital A. After she is stabilized, Betsy’s doctor recommends that she be discharge to her home with support for continued rehabilitation from PAC home health services. The home health agency (HHA) helps Betsy return to her home and coordinates care with multiple professionals and provider organizations including her primary physician, pharmacy, behavioral health provider, and outpatient dialysis provider. Home health nurses periodically complete formal Outcome and Assessment Information Set (OASIS) assessments per CMS requirements, tracking Betsy’s functioning as she recovers, including her mental functions, self care, and communication abilities.
Betsy has another medical event at home and is transferred to Hospital B. Based on evaluations performed at the hospital, Betsy’s doctors determine that she will need significant help to recover enough independence to return home and recommend transfer to a PAC skilled nursing facility (SNF). While admitted, the SNF completes Minimum Data Set (MDS) assessment instruments documenting Betsy’s abilities and progress. Once sufficiently recovered, the SNF discharges Betsy and she returns home with the help of a variety of home and community-based services (HCBS). While receiving HCBS, Betsy’s caregivers complete Functional Assessment Standardized Items (FASI) asssessments.
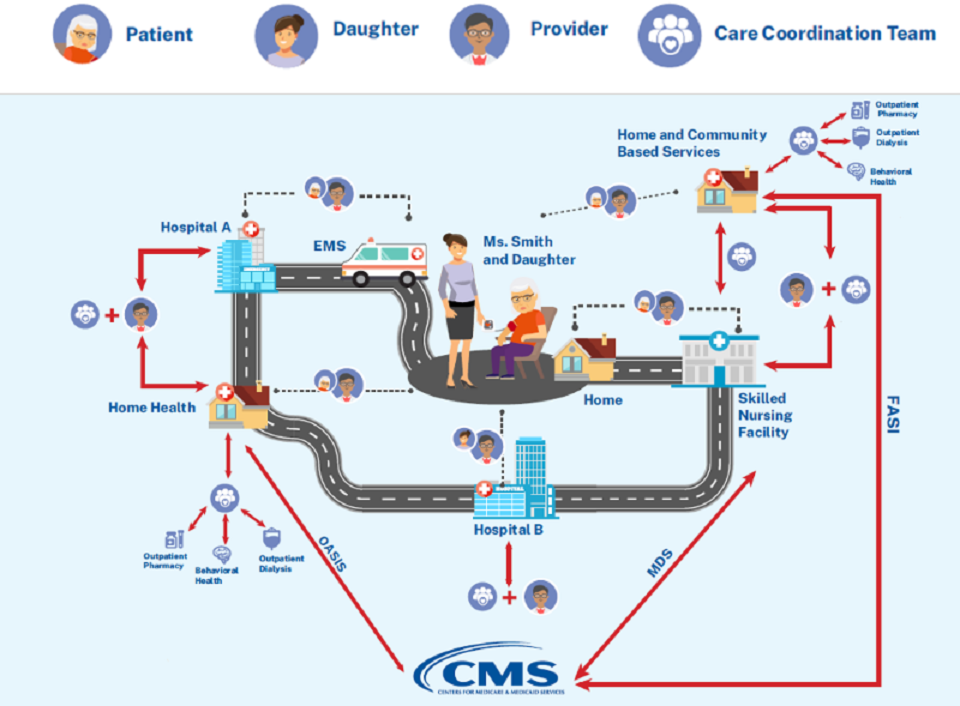
Figure 1: Example Post-acute Care Patient Healthcare Journey
Payers, such as Centers for Medicare & Medicaid Services (CMS), require formal assessments, such as the MDS within SNFs, to be performed and submitted in support of claims for provided services. Using the PFECollection and PFEObservation profiles, the electronic medical record (EMR) systems in which clinicians capture these formal assessments can electronically communicate the assessments to, or make them available for access by, payers. The same approach can be used to electronically communicate MDS assessments by SNFs, FASI assessments by HCBSs, OASIS assessments by HHAs, or other formal assessments. Note that this capability does not constitute a requirement to exchange assessments electronically with CMS or other payers.
When patients transition between facilities and care organizations, it is important for data collected about their functioning to follow them in order to enable appropriate care by the receiving facility. Using the PFECollection and PFEObservation profiles, the EMRs in which clinicians capture these formal assessments can electronically communicate the assessments to, or make them available for access by, the receiving facility and its clinicians. The same approach can be used to electronically communicate MDS assessments by SNFs, FASI assessments by HCBSs, OASIS assessments by HHAs, or other formal assessments.
Because transitions usually ocur between facilities of different types, e.g., SNF to HCBS, the recieving organization may not implement the specific assessments sent by the transferring facility. The categorization of observations into health domains defined by ICF enables recipients to prganize data for display based on the categorize even if the specific observation code is not known by their system.
Care provided by family members and caregivers outside of formal healthcare settings is an essential part of supporting individuals in regaining their functioning and independence. Making data available using the PFECollection and PFEObservation will allow FHIR-enabled applications that make data available to patients and their families to access information on their functioning. The categorization of observations into health domains defined by ICF enables these systems to present the information to users without understanding and implementing complex assessment tools.
IG © 2022+ HL7 Patient Care Work Group. Package hl7.fhir.us.pacio-pfe#1.0.0-ballot based on FHIR 4.0.1. Generated 2022-08-05
Links: Table of Contents |
QA Report
| Version History |
 |
Propose a change
|
Propose a change