
MCC eCare Plan Implementation Guide
1.0.0-ballot - Comment only
US
MCC eCare Plan Implementation Guide
1.0.0-ballot - Comment only
US
This page is part of the MCC eCare Plan Implementation Guide (v1.0.0-ballot: STU 1 Ballot 1) based on FHIR (HL7® FHIR® Standard) R4. The current version which supersedes this version is 1.0.0. For a full list of available versions, see the Directory of published versions
A Care Plan is a consensus-driven dynamic plan that represents a patient’s and Care Team Members’ prioritized concerns, goals, and planned interventions. It serves as a blueprint shared by all Care Team Members (including the patient, their caregivers, and providers), to guide the patient’s care. A Care Plan integrates multiple interventions proposed by multiple providers and disciplines for multiple conditions. A Care Plan may represent one or more Care Plans and serves to reconcile and resolve conflicts between the various plans developed for a specific patient by different providers. It supports the following use cases:
The vision of this implementation guide (IG), with the FHIR Care Plan profile as its framework, is to define a profile on the FHIR Care Plan resource that describes how it can be implemented and leveraged to support machine assisted care coordination between systems. It is assumed that SMART on FHIR Apps can be designed off of this guide to achieve that goal. The IG will also inform EHR systems on how to implement a structured encoded Care Plan.
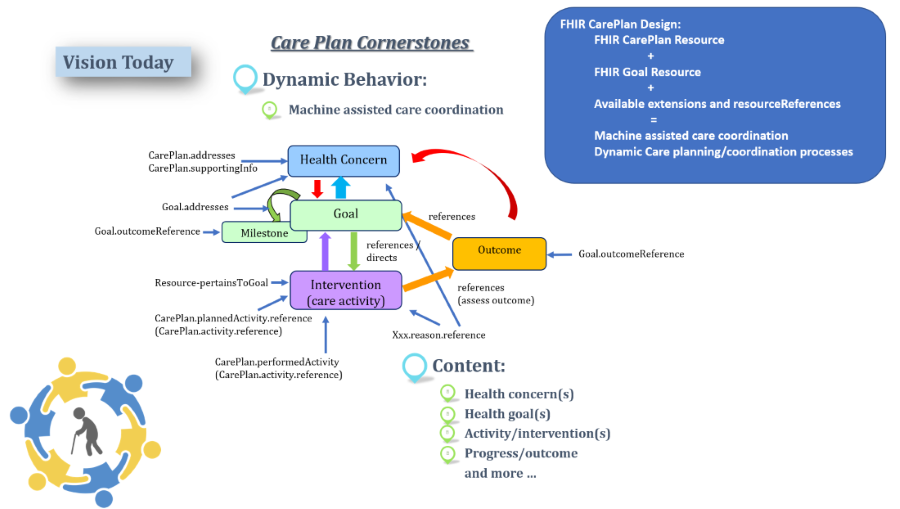
The dynamic care plan process diagram shows Care Plan Cornerstones as they exist within the clinical world and elements and attributes from the FHIR Care Plan resource structure that support the process. In order to encourage reuse and dynamic, machine assisted care coordination, the Care Plan profile design leverages referencing profiles wherever possible, especially within CarePlan.Activity.
 |
This profile on the FHIR Care Plan Resource describes rules, constraints to record, search, and fetch care plan data associated with a patient with multiple chronic conditions. It identifies which profiles, core elements, extensions, vocabularies and value sets SHALL be present in the resource when using this profile. Care plan data may or may not be tagged in an EHR as part of a care plan, but is also useful to retrieve data such as goals, problems, medications etc. and their time stamps from EHRs and other health system records to bring into an aggregated plan. This includes care plans that may be authored by a patient.
 |
The machine assisted dynamic care planning/coordination is supported in FHIR by leveraging together the Care Plan resource, the Goal resource, resource referencing and available extensions within those resources to link together the health concern or problem with its associated goals, interventions and outcomes. The intention is to re-use data entered in the EHR, whether it is in a Care Plan Application, or elsewhere in the EHR or other information system, rather than having a care plan be a double documentation burden. For example, if a procedure is ordered and performed and the health concern or problem reason for that procedure is asserted in the ordering workflow or documentation workflow - this information can be pulled into the Care Plan. If a goal is asserted for a patient outside of a care plan, along with the reason for that goal, this also can be pulled into a care plan. The Care Plan profile relies on referencing of profiles rather than “in-line” representation or documentation to enable a dynamic workflow and to be able to pull in and aggregate care coordination activities from disparate systems to provide a comprehensive care coordination view for patients.
CarePlan.Activity is a Backbone element. It identifies an action that has occurred, or a planned action. Represented with OUTCOME REFERENCE (performed activity) or ACTIVITY REFERENCE (planned activity)
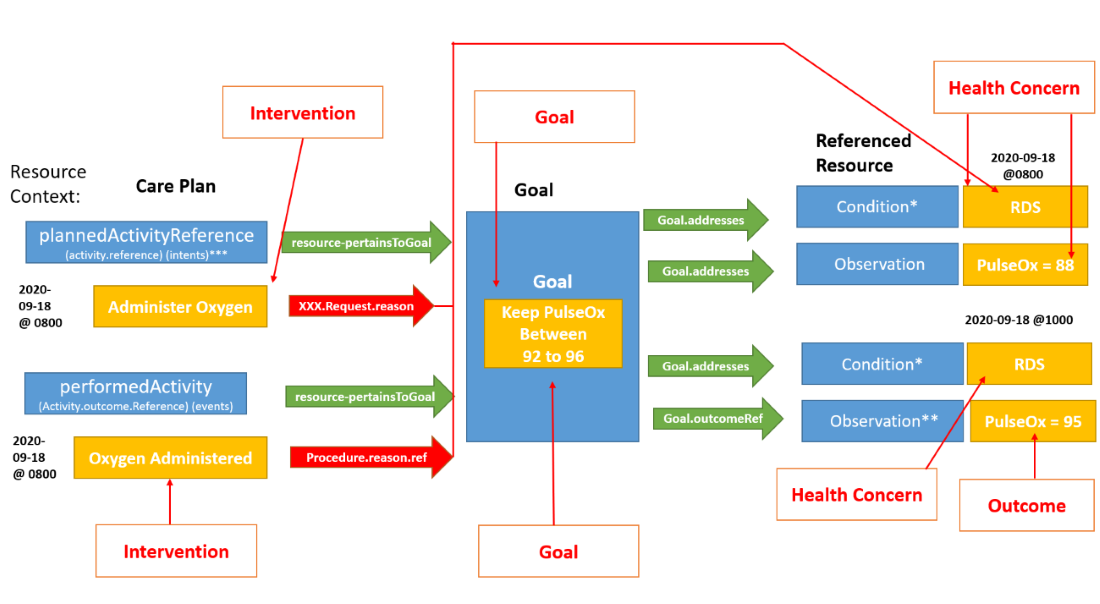
OUTCOME REFERENCE (aka PERFORMED ACTIVITY Reference): to be renamed in R5 to “CarePlan.performedActivity”. Please see https://jira.hl7.org/browse/FHIR-26064.) OutcomeReference is not only an outcome but rather an action such as a Procedure or an Encounter that was made or occurred or an Observation. Within CarePlan.performedActivity, the extension, “resource-pertainsToGoal” SHALL be used to reference this activity’s related goal. Within the resource referenced within performedActivity, “Procedure.reason” SHALL be used to reference the health concern or problem for which the activity is done.
ACTIVITY REFERENCE (aka PLANNED ACTIVITY reference): to be renamed in R5 to “PlannedActivityReference”. Please see https://jira.hl7.org/browse/FHIR-26064.) Within plannedActivityReference, the extension, “resource-pertainsToGoal” SHALL be used to reference this activity’s request’s related goal. “xxx.Request.reason” SHALL be used to reference the health concern or problem for which the activity is done. Within the referenced Goal resource, goal.address SHALL be used to reference the goal’s related Condition, Observation, MedicationStatement, NutritionOrder, ServiceRequest or RiskAssessment. Within the referenced Goal resource, Goal.outcomeReference, references the outcome (e.g observations related to the goal).
Health Concerns represented with:
Goals represented with:
Interventions represented with:
Outcomes represented with:
 |
This Care Plan aims to support care coordination and share relevant data across the care team, while avoiding double documentation. The IG describes referencing profiles and precludes using activity.detail due to its use of in-line representation which means that information would have been entered directly into a care plan module vs existing data being “pulled into” and aggregated within a dynamic plan. Please review the rules within the Care Plan Profile closely, as well as the explanatory text provided in the profile detailing what is required in both the Care Plan profile and each referenced MCC Profile. Please also review the library of value sets available for use within the MCC Profiles.
IG © 2020+ HL7 International - Patient Care WG. Package hl7.fhir.us.mcc#1.0.0-ballot based on FHIR 4.0.1. Generated 2022-12-04
Links: Table of Contents |
QA Report
| Version History |
 |
Propose a change
|
Propose a change