
Data Exchange For Quality Measures Implementation Guide
5.0.0 - STU5
![]()
Data Exchange For Quality Measures Implementation Guide
5.0.0 - STU5
![]()
This page is part of the Da Vinci Data Exchange for Quality Measures (DEQM) FHIR IG (v5.0.0: STU5 (v5.0.0)) based on FHIR (HL7® FHIR® Standard) R4. This is the current published version. For a full list of available versions, see the Directory of published versions
| Official URL: http://hl7.org/fhir/us/davinci-deqm/ImplementationGuide/hl7.fhir.us.davinci-deqm | Version: 5.0.0 | |||
| IG Standards status: Trial-use | Maturity Level: 4 | Computable Name: DEQM | ||
| Other Identifiers: OID:2.16.840.1.113883.4.642.40.23 | ||||
Copyright/Legal: Used by permission of HL7 International - Clinical Quality Information Work Group, all rights reserved Creative Commons License |
||||
This implementation guide defines a framework to support quality measurement, reporting, and related use cases by enabling the following capabilities:
Interoperability challenges have limited many stakeholders in the healthcare community from achieving better care at lower cost. The dual challenges of data standardization and easy information access are compromising the ability of both payers and providers to create efficient care delivery solutions and effective care management models. To promote interoperability across value-based care stakeholders and to guide the development and deployment of interoperable solutions on a national scale, the industry needs common information models and data exchange standards. The intent of the framework defined in this guide is to enable automatic data collection and submission limiting the need for manual processing and intervention. Ultimately, a national standard based on FHIR for data structure and exchange will reduce the burden on clinicians of transforming data between systems.
Although this implementation guide is US Realm, the framework is not realm-specific and much of the content is usable in other realms.
The guide is based upon prior work from the US Core and QI Core Implementation Guides and the QRDA Category I and III reporting specifications. Initially supported by the Da Vinci initiative, development and ongoing maintenance of this specification is managed by the sponsoring HL7 Clinical Quality Information (CQI) and Clinical Decision Support (CDS) workgroups and are incorporated as part of the standard HL7 balloting process.
This Guide is divided into several pages which are listed at the top of each page in the menu bar.
The following scenarios illustrate the various ways that the DEQM framework can be used, providing an overview of and index into the more detailed use cases and specification documentation in the implementation guide.
Broadly, these scenarios fall into three categories: 1) Reporting Scenarios, focused on communicating the results of a quality measure calculation at the end of a measurement period as part of a quality improvement initiative, 2) Exchange Scenarios, focused on echanging the data of interest for a measure or set of measures throughout the measurement period, and 3) Gaps in care scenarios.
As a precondition, systems in these scenarios have already obtained the relevant measure specifications being reported from a measure repository as described in the Quality Measure IG Measure Repository.
Reporting scenarios are used to report the results of quality measures on patient populations at the end of a measurement period. Measure reports are provided to attest the standard of care given to patients in a population as measured by specific quality measures. The measures are typically identified as part of a quality improvement initiative by a payer or other quality improvement stakeholder such as public health agencies with use cases that are typically more focused on the reporting scenarios.
For the reporting scenarios, the actors are Reporters and Receivers:
Reporters are the actors submitting the results of a quality measure. Depending on the reporting requirements for a particular scenario as well as the technical capabilities of the systems involved, the reporter may be different stakeholders such as providers, provider organizations, aggregators, or payers. In general, a reporter will consist of at least a Clinical Data Repository, the clinical system or systems containing information generated by or derived from the delivery of healthcare, and a Measure Evaluation Service, the system responsible for calculation of measure results.
Receivers are the actors receiving the results of quality measures. Again, depending on the reporting requirements and technical capabilities, receivers may be different stakeholders, but are typically aggregate-level stakeholders such as healthcare agencies, payers, and quality improvement organizations.
In each of these scenarios, the patients to be considered are determined by attribution. Since different quality initiatives may use the same measures with different attribution models, attribution is typically not specified as part of the measure specifications. The DaVinci Member Attribution List implementation guide supports the definition and exchange of member attribution lists as a potential approach to identifying patients to be considered for reporting.
In this scenario, a reporter such as a clinic submits a summary level quality measure report for a specific measure, attributed patients, and measurement period:

In this scenario, the resulting MeasureReport is a summary level measure report which includes only the population counts and calculated measure score. This scenario does not result in any patient-level data being communicated to the receiving system.
For more details on this scenario, see the Summary Reporting framework topic.
In this scenario, a reporter such as a hospital submits individual level quality measure reports for a specific measure and measurement period, for each attributed patient:

In this scenario, there is a Bundle of individual-level patient data for each attributed Patient. Determining the overall measure score then requires the additional step of aggregating the individual MeasureReport resources. Alternatively, a subject-list report can be included that references all the individual-level MeasureReports and provides the summary level measure score.
For more details on this scenario, see the Individual Reporting and Subject-list Reporting framework topics.
In each of the scenarios described above, the FHIR API is used directly to access the data of interest for the measure being reported. To support large volumes of data, Bulk Data may be used to transfer the data of interest between the clinical data repository and the measure evaluation service. As of the time of this publication, the Bulk Data specification is being updated to include important capabilities that will improve the performance of bulk data for the quality reporting use case, in particular the ability to organize bulk data feeds by patient. A future version of this publication will provide more detail on how this capability can be used directly once the updated Bulk Data specification is published.
In aggregated reporting, the measure calculation service gathers data of interest from multiple clinical data repositories, allowing for reporting in a variety of ways, including multiple facilities for a single provider, as well as multi-provider organizations:
Because data from multiple facilities and organizations can be aggregated in many ways; this specification is not prescriptive about how that aggregation is performed.
For simplicity, each of the above reporting scenarios is specified in terms of a single measure. However, all the framework operations and scenarios support specifying any number of measures to be reported. Reporting on multiple measures impacts:
In the simplest case, this approach identifies all the data required for calculation of any measure used in the quality initiative.
However, the approach also allows for submitting systems to choose which measures they are reporting, and determine only the data required for those measures.
For more details on data requirements, see the Data Requirements framework topic.
In addition to the reporting scenarios, Figure 1-4 illustrates Exchange Scenarios and their relationship to the Reporting Scenarios.
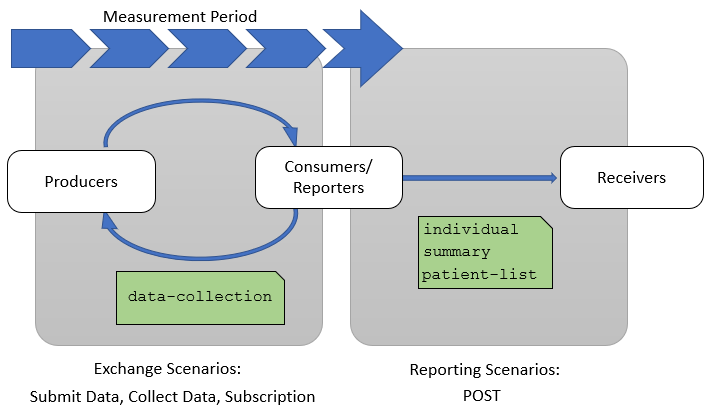
Exchange scenarios are used to exchange subsets of the data of interest for a measure or set of measures throughout the measurement period. These scenarios enable providers and quality stakeholders such as payers, accountable care organizations, and other secondary use partners to keep better track of how patients are performing with respect to a particular quality measure during the measurement period.
The three exchange scenarios are:
For these scenarios, the actors are Producers and Consumers, used in the same sense as the Producers and Consumers stakeholders in the Quality Measurement Standards Landscape diagram. Note that within any particular use case, different stakeholders will play the same roles. For example, a Provider may be playing the role of Producer in a particular exchange, while the Payer may be playing the role of Consumer.
Gaps in Care Reporting is a reporting scenario supported in this implementation guide. Similar to the quality reporting scenarios, a Gaps in Care Report is used to report the results of quality measures on patients or population, but for a gaps through period that is of interest for a Client.
The process below can be run as many times as useful during the reporting period to assure that all open gaps are closed.
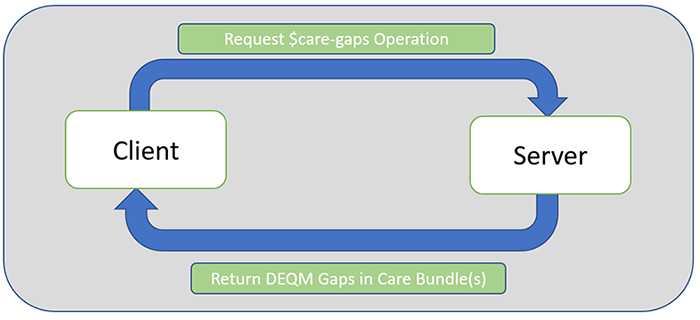
For the Gaps in Care Reporting Scenarios, the actors are Clients and Servers.
Clients are the actors requesting gaps in care results of quality measure(s). Depending on the reporting requirements for a particular scenario as well as the technical capabilities of the systems involved, the clients may be different stakeholders such as providers, provider organizations, aggregators, or payers. For example, if a provider requests a report from the payer's system, then the provider serves as the client. If a payer requests a report from their own system, they are the client.
Servers are the actors receiving the request for the Gaps in Care Report and producing it based on the information they have in their system. Again, depending on the reporting requirements and technical capabilities, receivers may be different stakeholders, but are typically aggregate-level stakeholders such as healthcare agencies, payers, and quality improvement organizations. For example, if a provider requests a report from the payer's system, then the payer's system serves as the server. If a payer requests a report from their own system, the payer's system serves as the server.
This Implementation Guide was made possible by the thoughtful contributions of the following people and organizations:
IG © 2020+ HL7 International / Clinical Quality Information. Package hl7.fhir.us.davinci-deqm#5.0.0 based on FHIR 4.0.1. Generated 2025-05-19
Links: Table of Contents |
QA Report
| Version History |
 |
Propose a change
|
Propose a change