
C-CDA on FHIR
1.2.0 - STU 1
![]()
C-CDA on FHIR
1.2.0 - STU 1
![]()
This page is part of the C-CDA on FHIR Implementation Guide (v1.2.0: STU 1) based on FHIR (HL7® FHIR® Standard) R4. This is the current published version in its permanent home (it will always be available at this URL). For a full list of available versions, see the Directory of published versions
This page provides a mapping from CDA to FHIR. For the FHIR to CDA mapping, please refer to Allergies FHIR → CDA. For guidance on how to read the table below, see Reading the C-CDA ↔ FHIR Mapping Pages
Uncommon use case: Multiple C-CDA Allergy Intolerance observations inside a single Allery Concern act should map to separate and distinct FHIR AllergyIntolerance resources. The C-CDA Companion Guide (see 5.2.7.1) actively discourages the practice of multiple osbervations insice a single act. It may occur, however, since Allergy Concern act allows for multiple Allergy Intolerance observations in C-CDA. Lossless transformations may not be possible without the use of extensions (see 3.1 of this guide).
| C-CDA¹ Allergy Concern act |
FHIR AllergyIntolerance |
Transform Steps & Notes |
|---|---|---|
| /statusCode | .clinicalStatus | For more information on how status is managed in Allergy Concern Act wrapper, refer to C-CDA guidance, see 5.2.7.1 Also see Status entryRelationship mapping below |
| All of the following are a Allergy Intolerance observation nested inside the Allergy Concern act. Each observation should become a distinct FHIR AllergyIntolerance resource. Include /entryRelationship[@typeCode=”SUBJ”]/observation prefix to rows below² |
||
| /@negationInd | See constraints under /participant | |
| /id | .identifier | CDA id ↔ FHIR identifier |
| /effectiveTime/low | .onsetDateTime | CDA ↔ FHIR Time/Dates effectiveTime/high should not be mapped within onset (DateTime or Period) |
| /value | .type & .category |
CDA coding ↔ FHIR CodeableConcept CDA value → FHIR type CDA value → FHIR category |
| /author | .recorder & Provenance |
Constraint: Only map single CDA author to FHIR recorder Guidance on CDA ↔ FHIR Provenance |
| /author/time | .recorded | Constraint: Only map earliest author/time CDA ↔ FHIR Time/Dates |
| /participant/participantRole/playingEntity/code | .code | Constraint: When CDA negation is absent or false CDA coding ↔ FHIR CodeableConcept |
| /participant/participantRole/playingEntity/code & /value |
.code | Constraint: When CDA negation is true and nullFlavor is used in playingEntity/code CDA No known allergy → FHIR code When negation is true and playingEntity/code is populated, use equivalent negated concept (e.g. map latex substance to no known latex allergy [1003774007, SNOMED CT]) if available. If not, use the substanceExposureRisk extension, placing the substance in the substance sub-extension and setting the exposureRisk sub-extension to no-known-reaction-risk. Note that when using this extension, the AllergyIntolerance resource will not be a conformant US Core AllergyIntolerance since the extension prohibits the required .code element. |
| Status /entryRelationship/observation[code/@code=”33999-4”]/value³ |
.clinicalStatus | CDA Allergy Status Observation value → FHIR clinicalStatus |
| Reaction /entryRelationship[@typeCode=”MFST”]/observation/value³ |
.reaction.manifestation | CDA coding ↔ FHIR CodeableConcept Both use SNOMED clinical findings with minor valueSet definition differences |
| Severity (nested inside Reaction) /entryRelationship[@typeCode=”MFST”]/observation/entryRelationship/observation[code/@code=”SEV”]/value³ |
.reaction.severity | CDA Severity value → FHIR Severity Note: CDA documents should not assign severity at the Allergy level. In cases where CDA assigns severity only to the Allergy rather than the reaction, map the severity to FHIR reaction severity, even if there are more than one. This means assuming that the same severity applies to all child reactions. If severity is assigned at both levels, the reaction level should be used. |
| Criticality /entryRelationship/observation[code/@code=”82606-5”]/value³ |
.criticality | CDA Criticality value → FHIR Criticality |
| Comment Activity /entryRelationship/act[code/@code=”48767-8”]/text³ |
Annotation .note |
1. XPath abbrievated for C-CDA Allergy Concern act as:
ClinicalDocument/component/structuredBody/component/section[code/@code=”48765-2”]/entry/act/
2. XPath abbrievated for C-CDA Allergy Inteolerance observation as:
ClinicalDocument/component/structuredBody/component/section[code/@code=”48765-2”]/entry/act/entryRelationship[@typeCode=”SUBJ”]/observation
3. Note that these entryRelationships will also have inversionInd=”true” in CDA
When authors or other provenance are recorded in the parent Allergy Concern Act, it is recommended that those data be mapped to the FHIR AllergyIntolerance.
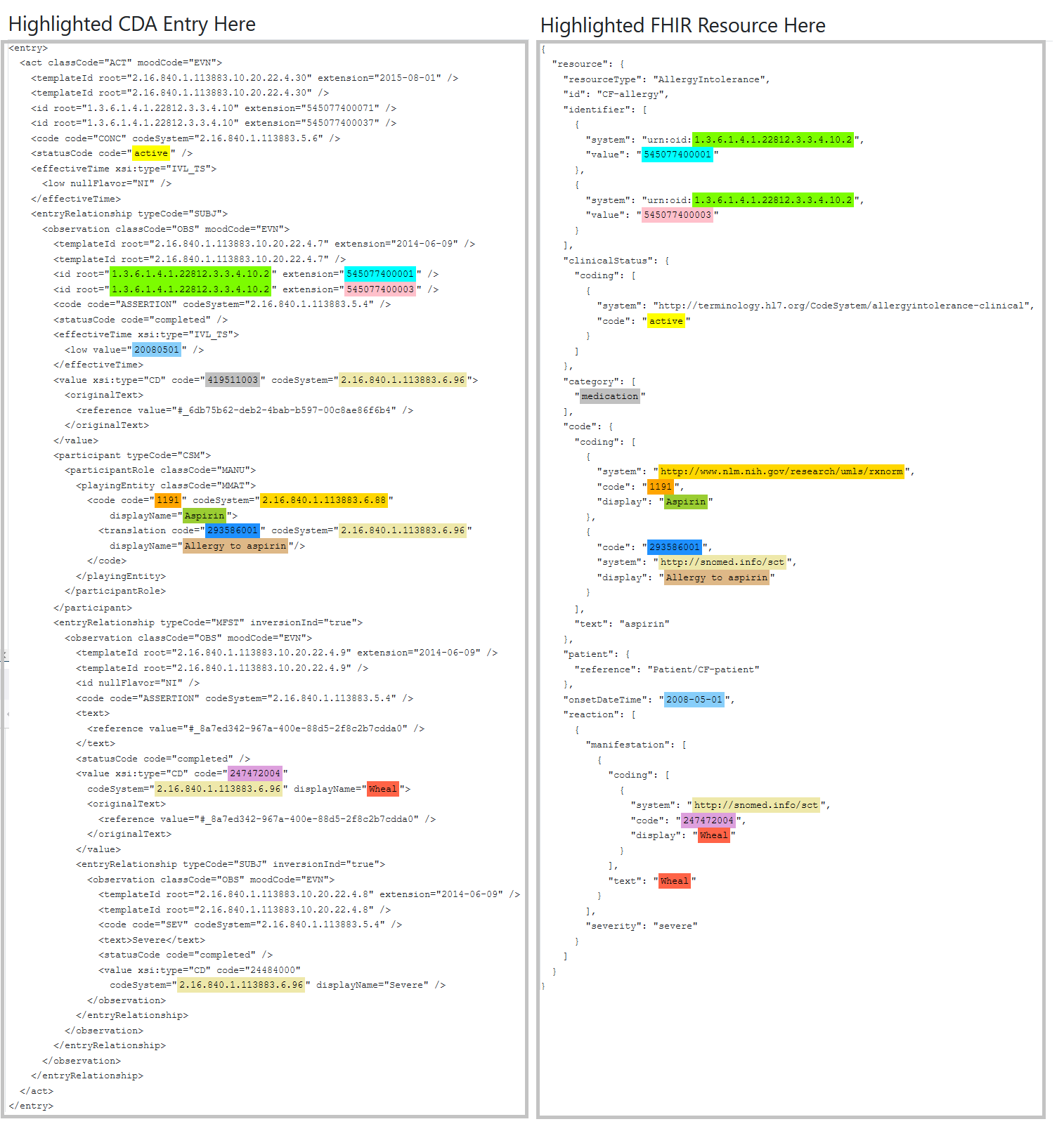
An illustrative example with highlighting is shown above based on the consensus of mapping and guidance. Not all possible elements in CDA or FHIR may be represented. To access the content for the above example, click on the links below.
The consensus mapping example developed through multiple vendors are available below:
As reviewed in the methodology, a more comprehensive review was performed via spreadsheets. These spreadsheets have been consolidated and further revised in the tables above but are provided for reference here
IG © 2020+ HL7 International / Cross-Group Projects. Package hl7.fhir.us.ccda#1.2.0 based on FHIR 4.0.1. Generated 2024-03-12
Links: Table of Contents |
QA Report
| Version History |
 |
Propose a change
|
Propose a change